Download
1 / 30
650 likes | 2.27k Vues
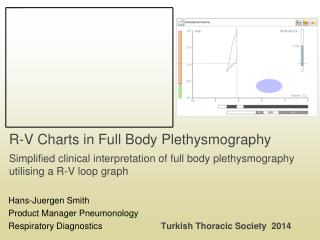
R-V Charts in Full Body Plethysmography Simplified clinical interpretation of full body plethysmography utilising a R-V loop graph. Hans-Juergen Smith Product Manager Pneumonology Respiratory Diagnostics Turkish Thoracic Society 2014. Limits of spirometry.

E N D
R-V Charts in Full Body Plethysmography Simplified clinical interpretation of full body plethysmography utilising a R-V loop graph Hans-Juergen Smith Product Manager Pneumonology Respiratory Diagnostics Turkish Thoracic Society 2014
Limits of spirometry • Forced breathing is UNEQUAL to tidal breathing • Flow limitation is UNEQUAL to obstruction • Degree of obstruction? • Small airways are not safely differentiated • Superimposing effects, dominance of central airways • Influence of the test itself • Deep inspiration (bronchoprotection, dilatation) • Functional and/or fixed conditions of the upper airways • Pain, cooperation, instruction Degree of severity? Character of disease?
Indications for full body plethysmography • Assessment of resting conditions • Little co-operation (peadiatrics, geriatrics, occupational medicine…) • Trend reports • Excellent intra-individual reproducibility CV% < 10% • Grading and differentiation • Objectivation of limitation (stage of disease) • Differentiation between obstruction and restriction • Distribution of obstruction (extra thoracic, central, peripheral) • Inhomogeneity of the lung • Bronchial hyperresponsiveness • Degree of reversibility • Challenge testing (+PC/D 100 for sRaw) • Prognosis • Expert report
Workflow of examination 3 standardised methods (manoeuvres) • Recording of sRaw breathing loops • a) Determination of FRCpleth (ITGV) b) “linked” manoeuvre: FRCpleth + spirometry • Forced spirometry (Slow spirometry) • Fixed in the order • Manoeuvres can be skipped • Manoeuvres can be repeated
1. Tidal breathing: Measurement of sRaw V‘ [L.s-1] Parameters DV‘ Flow sReff sRtot Raw DVbox Shift volume TGV Vbox[mL] DVL The loop of specific resistance incorporates resistive and volume determined components, not differentiated.
Specific airways resistance (sRaw) Test sequence (assistant): • Box door firmly closed! • Automated loop compensation activated • Instruct spontaneous breathing without preconditions • Wait until patient is adapted to the unit – reproducible loops after 3 to 5 breathing cycles • Loops can be stored as soon as they are reproducible • Low variation of approximation line (sRaw) and small loop area • In case of small specific resistance values (steep loops), instruct slight hyperventilation with BF 20-25 min-1 Quality control: • Wait for regularity of compensated loops; regular BF and VT • Store the last 5 loops of specific resistance by activating the shutter (determination of the FRCpleth)
SentrySuite body application – measurement mode • Workflowconcept • Guidance • Resting breathing on FRCprior to shutter manoeuvre • FRC stability • VT stable • BF stable • Lowest WOB • Automated recording of breathing loops Breathing loops FRC stability at tidal breathing
2. Shutter: Determination of FRCpleth Parameter Pm [kPa] DPm Occlusionpressure FRCpleth(ITGV) Raw DVbox Shiftvolume FRCpleth Vbox[mL] DVL Determination of intrathoracic gas volume on the level of FRC
Intrathoracic Gas volume FRCpleth Test sequence (assistant): • After activation of the FRC-measurement, the shutter is automatically closed at the beginning of the following inspiration (FRC-, ITGV-level) • Patient should continue normal breathing, without additional effort against the shutter • Shutter should not be „blown up“ or „soaked-up“ by the patient • Lips must be firmly closed at the whole manoeuvre • Record at least 2 shutter manoeuvres which were not influenced by a deep inspiration, as the deep inspiration can alter the FRC as well as the sRaw
Workflow body – linked manoeuvre Resting breathing - shutter linkedwith SVC Volume IC VCex Shutter RV ERV VT IRV FRCpleth FRC-stability ERV VCin FRC TLC RV Time In linked manoeuvre – patient should not release mouthpiece!
SeS body application window Breathing loops and shutter curves • Breathing loops from tidal breathing • Panting or resting breathing at FRC shutter manoeuvre • Shutter Linked with slow or forced spirometry; started with • IC • ERV • Flow-volume-loops Shutter curves Breathing loops
DuBois Plethysmograph 1956 1. Oscilloscope sRaw, FRCpleth 2. Oscilloscope Cl, Rl Plethysmography according to DuBois Measurement ofresistance Measurement oflung volume
DuBois, Goldman- Analysis of breathing loop Vogel - Index of non-homogeneity RE‘/RE0 Ulmer - Volume dependence of Raw Intra-breath analysis on Raw proximal obstruction distal obstruction normal stenoses sRE‘ sRaw sRaw sRaw sRaw sRE0 Islam MS, Ulmer WT. Der Strömungswiderstand in den Atemwegen und das Lungenvolumen. DtschmedWochenschr 1977; 102 (33): 1187-1190 (Dependenceofairwaysresistance on lungvolume.)
R-V analysis according to Ulmer Islam MS, Ulmer WT. Der Strömungswiderstand in den Atemwegen und das Lungenvolumen. Dtsch. Med. Wschr. 1977; 102: 1187-1190 (Dependence of airways resistance on lung volume.)
Resistance-volume transformation Instantaneous course of resistance Breathing loops Airways resistance - central R-V loop R-V transformation DRaw Predicted area Raw FRCpleth FRCpleth linked with SVC Absolute lung volumes - peripheral
Resistance-volume chart (R-V chart) • Combination of relevant clinical parameters • Raw (Rcent, Reff, Rtot…) • FRCpleth • Linked SVC (TLC, RV…) • Predicted area • Intra breath pattern of Raw • Volume dependence • Flow dependence • Dynamic range Normal | abnormal airways resistance R-V loop DRaw Predicted area Raw FRCpleth Actual Predicted Absolute lung volumes
Weibel: Morphometry of the human lung Cross sectional area [cm²] 2.5 2.0 5.0 1.8 x 10² 9.4 x 10² 5.8 x 10³ 56 000 000 Resistance [kPa/(L/s)] 0.05 0.05 0.02 Genera- tion 8-10 17 24 Larynx Trachea Bronchi Bronchioles Alveolar Ducts Alveoli Central airways Raw ~ 80% Peripheral airways Raw < 20% TGV > 60 % Weibel, Morphometry of the Human Lung, Springer 1963
Application screen menu R-V chart R-V chart differentiating Raw and TGV Breathing loops Conventional sRaw breathing loops incorporating Raw and TGV
Within breath dynamics of Raw New, additional information, if requested. Phenotyping of obstruction Small airways diagnostics! Volume type (COPD) D between end-expiration and end- inspiration Flow type (asthma) D between no-flow and maximal-flow Begin of inspiration
R-V pattern Exhalation Inhalation normal flow type end-expiratory closing volume type central obstruction obesityperipheral obstruction
Pre-post assessment (conventional) Resistance? Lung volumes? Abnormality? Reversibility? Flow type? Volume type? PrePost Shutter curves Pre Breathing loop Post Parameter table is needed !
Comparison COPD Restriction Obstruction & end-expiratory inhomogeneity Obesity Obstruction Obstruction & Hyperinflation Combined obstructive restirictivedisease RV loop Restriction Hyperinflation
R-V charts summary Routine measurement not effected – report Recommended interpretation is kept! Simplified clinical oriented report • Relation between Raw and lung volumes • Visual diagnostics based on normal range • Differentiation between central airways and/or peripheral airways • Phenotyping / Small airways diagnostics • Volume type – COPD • Flow type – asthma • Most powerful features • Pre-post assessment, hyperresponsiveness • Differentiated presentation of reaction in Raw, lung volumes or combination