Download
1 / 64
700 likes | 1.5k Vues
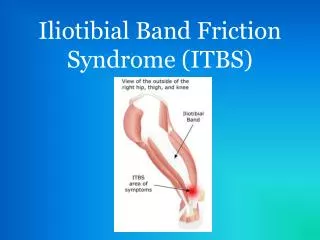
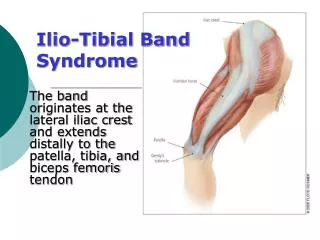
Iliotibial Band Friction Syndrome. What is it?. Pathophysiology. The iliotibial band (ITB) is a dense fibrous band of tissue that originates from the anterior superior iliac spine region and extends down the lateral portion of the thigh to the knee.

E N D
Pathophysiology • The iliotibial band (ITB) is a dense fibrous band of tissue that originates from the anterior superior iliac spine region and extends down the lateral portion of the thigh to the knee. • The ITB has insertions on the lateral tibial condyle (ie, the Gerdy tubercle) and the distal portion of the femur. • When the knee is extended, the ITB is anterior to the lateral femoral condyle. • When the knee is flexed more than 30º, the ITB is posterior to the lateral femoral condyle. See the images below.
Frequency • Iliotibialband syndrome (ITBS) is most common in athletes who participate in long-distance running. Studies have indicated a 4.3-7.5% occurrence rate for ITBS in long-distance runners. • ITBS is less common in shorter-distance or sprint-distance runners. • The higher rate in long-distance runners is primarily because of the increased stance phase during longer-distance running. • ITBS also has been reported in military recruits, cyclists, and tennis players. • The frequency of ITBS is also increased in adolescents undergoing the rapid growth phase
Race No known association exists between race and iliotibial band syndrome. Sex • Iliotibial band syndrome has been reported in men and women equally; however, women may be more susceptible to developing the syndrome because of anatomical differences of the thigh and knee, such as genu varum and increased internal tibial rotation. These anatomical differences result in weakness of the quadriceps muscle and an increased varus angle of the femur in relation to the knee. Age • Iliotibial band syndrome usually is seen in individuals aged 15-50 years, an age range that generally includes active athletes.
Bands acts to coordinate muscle function and stabilize the knee during running
The patient with iliotibial band syndrome typically reports pain at the lateral aspect of the knee; • In some cases, the presenting symptom is hip pain over the greater trochanter. • The pain usually worsens with physical activity, such as running or cycling. • Pain may be exacerbated by running hills and is most intense at heel-strike. • Some patients may also report lateral knee pain when walking up or down stairs. • The patient also may report an audible, repetitive popping noise in the knee with walking or running.
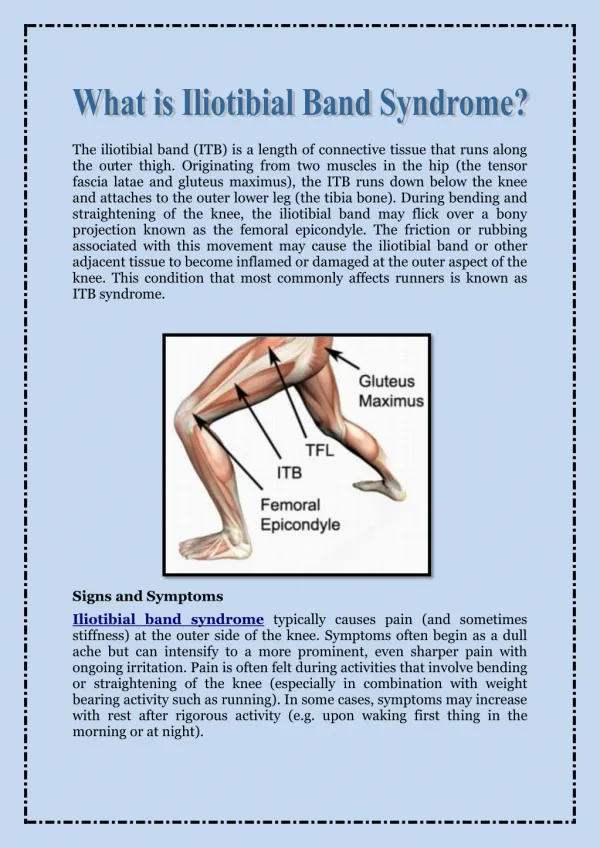
(ITBS) is the result of inflammation and irritation of the distal portion of the iliotibial tendon as it rubs against the lateral femoral condyle, or less commonly, the greater tuberosity. • Thisoveruse injury occurs with repetitive flexion and extension of the knee. Inflammation and irritation of the iliotibial band (ITB) also may occur because of a lack of flexibility of the ITB, which can result in an increase in tension on the ITB during the stance phase of running.
Physical • The physical examination should include the entire lower extremity to rule out other causes of lateral knee or hip pain. • In most cases, point tenderness occurs with palpation of the lateral femoral condyle or lateral tibial condyle, especially when flexing or extending the knee, as the iliotibial band (ITB) slides across the lateral femoral condyle. • Some patients may have tenderness over the greater trochanteric region of the hip.[5] • Strength testing - Strength testing may reveal knee flexor or extensor weakness or hip abductor weakness. • Tests - Increased or noticeable tightness of the ITB also may be noted upon examination with the Ober test. • A modified Thomas test can be performed to assess flexibility of the hip flexors, hamstrings, and ITB.
Ober Test Ober test assess the flexibility of the ITB tensor fascia lataeand gluteal muscles
Noble Compression Test • Place thumb over lateral femoral condyle • Flex and extend the knee • Jump off the table with 30 degree of flexion
Causes • Iliotibialband syndrome (ITBS) typically is due to overuse. • The injury is seen most commonly in runners, although other athletes (eg, cyclists, tennis players) also may be affected. • The usual mechanism is irritation of the iliotibial tract as it crosses over the lateral femoral condyle and, less commonly, the greater tuberosity. • Increased tension or friction of the ITB in this area can result in an increase of irritation or inflammation. • Abnormal gait or running biomechanics also have been implicated. • Cyclists may experience ITBS due to improper positioning on their bike. Excessive internal or medial rotation of bike cleats and a bike seat that is too high are 2 main causes of ITBS among cyclists.
Long-distance runners have a higher incidence of ITBS than do short-distance runners and sprinters. This higher incidence may be due to the change in the biomechanics of running versus sprinting. • Long-distance runners tend to have a more prominent and extended heel-strike and stance phase in comparison with sprinters. • The ITB is under its greatest tension during the first third of the stance phase. • Weakness of muscle groups in the kinetic chain may also result in the development of ITBS. • Weakness in the hip abductor muscles, such as the gluteus medius, may result in higher forces on the ITB and the tensor fascia lata.
Differentials • Hamstring Strain • Medial Collateral and Lateral Collateral Ligament Injury • Meniscal Injury • Myofascial Pain • Osteoarthritis • Overuse Injury • Patellofemoral Syndrome • Trochanteric Bursitis
Laboratory Studies • Laboratory studies are not indicated for the diagnosis of iliotibial band syndrome. • However, laboratory tests may help rule out other sources of knee pain, such as rheumatoid arthritis or a septic joint.
Imaging Studies • Imaging tests are not necessary to confirm the diagnosis of iliotibial band syndrome (ITBS). • Depending on the findings of the physical examination, the physician may want to obtain radiographs of the knee to rule out other pathology such as a fracture or bone spur.
Imaging Studies • In severe cases, magnetic resonance imaging (MRI) may be helpful in identifying the extent of inflammation of the ITB. • Findings on MRI most commonly include thickening of the ITB in the region overlying the lateral femoral condyle and fluid collection underneath the ITB at this area.
Physical Therapy • Treatment for iliotibial band syndrome (ITBS) usually is conservative. Conservative treatment consists of • (1) relative rest by decreasing the amount of exercise or training, • (2) the use of superficial heat and stretching prior to exercise, and • (3) the use of ice after the activity. Heat should be applied before and during stretching for at least 5-10 minutes, and ice treatments should be employed using a cold pack applied to the area for 10-15 minutes or using an ice massage, which involves rubbing ice over the inflamed region for 3-5 minutes or until the area is numb.
Physical Therapy • in addition to reducing the amount of inflammation and irritation. • The physical therapist can advise the athlete about ways to modify his/her training program so that faster results are seen with therapy. • Running and cycling should be decreased or avoided to prevent further repetitive stress to the ITB. • Wearing proper shoes also is very important in individuals with ITBS. • Frequently, patients with ITBS demonstrate excessive pronation of their feet. • The physical therapist should evaluate the patient's biomechanics during walking and running and should assist him/her in obtaining custom-made orthotics to correct faulty mechanics that may be causing the ITBS.
Physical Therapy • Wearing proper shoes also is very important in individuals with ITBS. • Frequently, patients with ITBS demonstrate excessive pronation of their feet. • The physical therapist should evaluate the patient's biomechanics during walking and running and should assist him/her in obtaining custom-made orthotics to correct faulty mechanics that may be causing the ITBS.
Physical Therapy • Physical therapy treatment in the acute stage may include modalities such as phonophoresis or iontophoresis in addition to cryotherapy to decrease the inflammation. • Since some cases of ITBS are caused by excessive tension on the ITB, physical therapy can help to incorporate proper stretching techniques into the patient's exercise routine.
Physical Therapy • These exercises concentrate on increasing flexibility of the ITB and of the gluteus muscles. • Other muscles that commonly need attention for flexibility include the hamstrings, quadriceps, gastrocnemius, and soleus
Soft-tissue mobilization and massage techniques may be used to assist with lengthening of the sore ITB. • Prior to mobilizing the tissues, the physical therapist may perform an ultrasonographic treatment over the ITB to increase blood flow to the area and prepare the tissues to be stretched. • Massage should generally be performed with the ITB in a lengthened state.
Physical Therapy • As the patient's symptoms improve, the physical therapy can progress toward strength development and maintenance. • The physical therapist should instruct the patient in a home exercise program that continues to improve the strength and endurance of the hip and knee, as well as the back and abdominals. • Strengthening of the hip abductors and knee flexors and extensors is an important component of rehabilitation. • Once the patient is able to complete all strengthening exercises without discomfort, he/she may gradually return to the previous training regimen.
Stretch #1: Pull foot up to back of buttocks. Cross the uninjured leg over the injured leg and push down, hold for 30 seconds.
stretch #2:Cross injured leg behind and lean towards the uninjured side. This stretch is best performed with arms over the head, creating a "bow" from ankle to hand on the injured side (unlike how it is depicted).
Stretch # 3:Cross injured leg over the uninjured side and pull the leg as close to your chest as possible.
Foam Roller (left and below): Roll your injured leg over the foam roller, add more time gradually each day to help mobilize your tissues and break up scar tissue.
Balance on 1 Leg Strengthening (left and below): May start just balancing on one foot when brushing your teeth. Gradually you can add challenges such as using a soccer ball and moving the ball in different directions. Another good method is to balance on one foot and play catch with yourself with a tennis ball against a wall or dribble a basketball. Start out with one minute at a time, and build up to 3-5 minutes.
Side Leg Lifts:Keep the back of the leg and buttocks against the wall. Slide the leg up the wall and hold at the top for 5 seconds then slide back down. Point toes down.
Start with one set of 20 each leg, after 1 week add a second set of 5. Every 2 days add 5 more as long as it is being well tolerated until you build up to 3 sets of 20 lifts
Strengthening with Theraband (left and below): Loop one end and close in the door. Loop other end around the uninjured leg. Bend your knee on the injured leg and balance on the injured leg. Put your uninjured leg through a range of running motion, going up and back. Build up to 3-5 minutes, make sure to exercise both legs.
Occupational Therapy Occupational therapy usually is not indicated in the treatment of individuals with iliotibial band syndrome.
Surgery • If the patient still does not improve, then tendon-lengthening surgery with excision of the damaged ITB may be required. • Surgery for the correction of ITBS has typically been an open procedure using a Z-plasty technique, although small prospective studies have used arthroscopy to create a diamond-shaped defect in the ITB.