Download
1 / 22
220 likes | 325 Vues
The VTE Symposium held on 21st September 2010, led by Dr. Tamara Everington, focused on the challenges in achieving compliance with NICE quality standards for VTE risk assessment. It discussed critical strategies, such as staff education, electronic systems, and the documentation of repeated risk assessments. Additionally, the symposium explored the importance of offering appropriate VTE prophylaxis and effective communication with patients. Attendees engaged in discussions on improving clinical practices to address VTE risks, aiming for a substantial reduction in secondary VTE incidents.

E N D
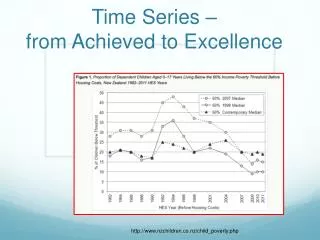
What still needs to be achieved in the clinical situation? VTE Symposium – sharing good practice 21st September 2010 Dr Tamara Everington
What is your background? • Doctor • Nurse • Pharmacist • Risk Manager • Executive • Other
NICE Quality Standard 1 • “All patients, on admission, receive an assessment of VTE and bleeding risk”
Which 1 of these do you think is most likely to increase compliance with VTE risk assessment? • CQUINS targets • Executive Drivers • Better staff education • Electronic Systems • Productive Wards
NICE Quality Standard 2 • “Patients are re-assessed within 24 hours of admission for risk of VTE and bleeding”
How should you document repeat VTE RA at 24 hours? • Repeat the initial VTE RA document • Document in the clinical pathway (PTWR) • Pharmacy check • Nurse check • Other
NICE Quality Standard 3 • “Patients assessed to be at risk of VTE are offered VTE prophylaxis in accordance with NICE guidance”
Which groups would you adjust thromboprophylaxis dose in? • Renal impairment • Obesity • Cancer patients with cachexia • Recurrent “fallers” • All of the above • None of the above
Which day cases do you plan to risk assess? • Day surgery under GA • Day surgery under LA • Fracture clinic • Chemotherapy patients • Medical day cases • 1,(2), 3 & 4 • All of the above
How will you pick up secondary VTE? • Via anticoagulant referrals • Via radiology reports of VTE • Via clinical coding • Via death certificates • Via the Coroner • Combination of the above?
NICE Quality Standards 4 & 5 • “Patients / carers are offered verbal and written information on VTE prevention at time of admission…. & as part of the discharge process”
Simples!!!! If only!!!
What information is most likely to work? • Written information • Visual information • Face-to-face explanation • A mixture of the above
NICE Quality Standard 6 • “Patients provided with anti-embolism stockings have them fitted and monitored in accordance with NICE guidance”
Which of the following have you seen on patients? • Which of the following have you seen on patients? • Stockings causing a ‘tourniquet’ effect • Damaged legs from stockings • Soiled stockings • All of the above • “I wish you hadn’t asked that question”
NICE Quality Standard 7 • “Patients receive extended postoperative VTE prophylaxis in accordance with NICE guidance”
A 65 year old woman with a history of VTE has incurable ovarian cancer with reduced mobility which can be controlled with indefinite chemotherapy. • Not at all • Aspirin only • For 28 days following surgery • Indefinitely How long would you continue thromboprophylaxis?
Which method of RCA do you think will be most effective? • RCA by the Thrombosis Committee • RCA by the VTE nurse • RCA by Clinical risk • RCA by Clinical teams