Download
1 / 17
170 likes | 298 Vues
Mental Health, Genomic Medicine and Patient Care for our Veterans Gerry Higgins, M.D., Ph.D.; Facilitator Chair, Genomics Advisory Panel, OSHERA. TOPICS. Mental Health Services – Challenges: → Suicide → Post-Traumatic Stress → Treatment-resistant depression

E N D
Mental Health, Genomic Medicine and Patient Care for our Veterans Gerry Higgins, M.D., Ph.D.; Facilitator Chair, Genomics Advisory Panel, OSHERA
TOPICS • Mental Health Services – Challenges: → Suicide → Post-Traumatic Stress → Treatment-resistant depression → Poly-pharmacy and comorbidity 2. The Importance of the Million Veteran Program and Genomic Medicine at the VA 3. Integration of Genome Data into the VA’s EHR: → Why it is important for the individual Veteran → Update, challenges and risks
Rank order, Top Health Care Challenges in the Veterans Health Administration; • Survey of 67 VA Clinicians, All Specialties at 24 Sites:1 • Treatment-Resistant Depression • Treatment-Resistant Anxiety • Traumatic Injury • Addiction / Alcoholism • Posttraumatic stress • Cardiovascular Disease • Oncology • Gastroenterology • Dementia • Sleep Disorders • Conducted by Liberty Mutual Patient Safety Institute under contract with the VHA.
Challenges - Suicide →“Suicide rates among Veterans treated in the VA System are about 50% higher than in the general population, and the rate of suicide among active duty service personnel has recently exceeded the rate in the general population.” →From DoD Suicide Event Report Program (2008-2010):
Challenges - PTS → Using the strictest PCL criterion for OIF/OEF Veterans → Time-course using DSM-5 ‘Experiencing’ criteria *5.2% after 20 years
Challenges – Treatment-Resistant Depression →Major depressive disorder (MDD) strikes 14% - 17% of Americans during their lifetime. → >30% of individuals with MDD do not achieve remission after 4 long antidepressant trials. → 22% of Americans view MDD as a ‘personal weakness.’ → MDD costs the U.S. economy an estimated $150 B each year. →Co-morbidities: CARDIO MDD SUICIDE PTS
Goals of VA Genomic Medicine Program • Collect and link genetic information with VA Electronic Health Record and thereby: • Discover genetic predispositions,causes and mechanisms of disease • Better define treatments • Pharmacogenomic & interventional customization • Via research, advance understanding in all these areas • Establish how genetic information will be used in clinical medicine • Translational research to link genotype to phenotype • Complex, adult, multi-gene diseases possibly with strong environmental influences • The Million Veteran Program • ‘Whole genome sequencing & analysis’ to provide largest study of disease associations and human genetics • Will help all studies examining how genome variants lead to disease and help understand gene x environment interactions
Breakthroughs in Epigenomics may lead tounderstanding of how combat stress leads to PTS Epigenomics: A genomic approach to studying environmental effects, primarily DNA methylation, on gene function. Repetitive combat stress causes Epigenomic changes to genes in the stress response
Breakthroughs in Epigenomics may lead tounderstanding of how combat stress leads to PTS Combat stress → Prolonged stress Hypermethylation of PTS response glucocorticoid receptor
Breakthroughs in Epigenomics may lead tounderstanding of how combat stress leads to PTS • →Patients with PTSD have increased plasma levels of cortisol, show a dysfunctional cortisol rhythm, and an exaggerated stress response. Plasma Cortisol
Clinical Decision Support in the EHR - Only First Phase of Omic Integration into EHRs
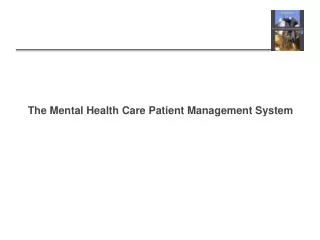
Architecture for Pharmacogenomic Decision Support1: • Infrastructure Overview of Required Elements Pharmacogenomic Decision Support Resources CDS Pre-Requisites Centrally managed repositories of medical knowledge 2. Standardization of CDS information for genomic medicine 3. Standard approach for representation and locating patient data Computer processable medical knowledge Computer-interpretable patient data Generation of patient-specific advice using knowledge and patient data → Rules Engine → MLM → Machine Learning component such as Support Vector Machine (SVM) → Remote web access input 1Based on: Kawamoto K et al. A national clinical decision support infrastructure to enable the widespread and consistent practice of genomic and personalized medicine. BMC Medical Informatics and Decision Making. 2009; 9:17 doi:10.1186/1472-6947-9-17.
Architecture for Advanced Pharmacogenomic Decision Support: • What’s Missing? Drug – Gene Interactions (DGIs) • → Here are some reasons that the DGI domain has not received the focus it deserves: • Drug-drug interactions are difficult to model, except in a generic manner, and once the algorithm has to handle many drug pairs (i.e., >2) it becomes an impossible combinatorial problem – especially as poly-pharmacy seems to be on the rise. To add a patient's variable metabolizer phenotype into the math, and the problem becomes intractable. • The advent of next generation sequencing (NGS) has changed everything. Every vendor is very concerned that maintenance and upgrades will require tremendous resources to keep up with the very rapidly world of ‘omics. • Physicians are already upset about medication alert fatigue, and since they were never thoroughly educated in genomics or pharmacogenomics, vendors are uncertain about how to proceed. In addition, both professional medical organizations and payors are still somewhat skeptical about gene testing.
Preemptive Genotyping Obtain known actionable pharmacogenomic variants for each patient using multiplexing / NGS panels Store pharmacogenomic data in EHR High Risk Patients in Medical Home EHR system automatically provides physician with optimal therapeutic regimen for patient Advanced pharmacogenomic decision support Trigger Search for pharmacogenomic data in patient’s EHR Inpatient Gets New Prescription Find possible risk variant
Possible integration of omic data directly into the VistA electronic health record • How could this be achieved? 2. Since epigenomic data, which has been highly replicated, shows a correlation between hyper-methylation of the glucocorticoid receptor and PTS (as well as MMD and BPD) – how can we integrate these data? 3. What concerns do Veterans have about protection of personal privacy in this rapidly moving domain?
END OF PART ONE: Questions? Discussion?