Download
1 / 18
180 likes | 274 Vues
This study analyzes corruption in local health care provision in Bolivia, focusing on voice and accountability. The research explores management practices and covariates of corruption using newly collected data. Findings indicate the impact of informal payments on perceived corruption. The implications suggest improvements in management practices and the importance of active community engagement.

E N D
Determinants of Corruption in Local Health Care Provision:Evidence from 105 Municipalities in BoliviaRoberta Gatti, George Gray-Molina and Jeni KlugmanFebruary 18th, 2004
Objective: analyze the determinants of corruption in the health sector at the local level with particular focus on issues of voice and accountability. Context: Part of a larger project that investigates the impact of decentralization on human development outcomes (in particular health) in Bolivia Methodology: cross-sectional regressions at the municipality level
Why the focus on local level delivery of health care? Two relevant reforms introduced in the 1990s: • Seguro Basico de Salud (1996 and 1998) • Decentralization reforms: Law on Popular Participation, 1994
Why the focus on corruption? • International evidence on consequences of corruption suggests corruption is associated with lower investment, growth, and lower share of education and health spending (see eg Mauro, 1995; 1998); • Bolivia scores poorly in reviews of governance (see eg Trasparency International)
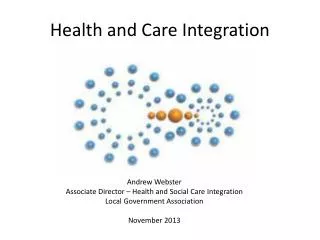
Central Government (MOH) Local Government Funds/Appointments Deconcentrated Institutions Media, local org. Information Public Hospital Services Local Electorate Private Hospital (exit option) voting Funds/appointments voting
Determinants of corruption The literature on determinants of corruption identifies a number of correlates of corruption (level of development, degree of competition, participation of women to public life, decentralization, etc.). • Most of the findings in the literature are based on cross-country, cross-sectional data • There is anecdotal evidence that voice and accountability could keep corruption in check but this hypothesis has not been tested systematically so far
How do we measure corruption? Related work (Chakraborty et al. 2002) • Informal payments for services that are meant to be rendered for free. There we find that 30% of respondent pay on average $5 for procedures that are supposed to be free.
This paper focuses on the perceptions of corruption by health care users
The data Newly collected data from three sources: • health facilities • health service users (2000 users in 108 municipalities) • municipal government (108) Municipal sample stratified by two criteria: i. new/old municipalities ii. urban/rural.
What is our focus in studying the covariates of corruption? Mechanisms for accountability • Exit/Voice • Management Practices
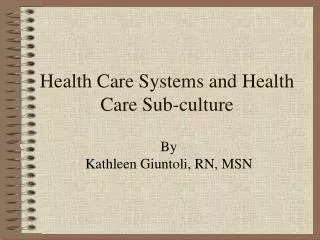
Variable Obs Mean Std. Dev. Min Max Corruption 108 2.17 .32 1.23 2.83 Labor per capita income (annual) 108 2795.23 1325.59 798.64 7702.79 Total per capita income (annual) 108 3071.06 1472.19 798.64 8585.50 Illiteracy rate (1995) 108 .74 .14 .28 .95 Waiting time 108 1.25 .18 1 1.9 Distance to hospital 108 1.18 .21 1 2.25 Percent rural population 106 .70 .34 0 1 Summary Statistics (Table 2) Income is in Bolivianos, 2001. Waiting time:1=less than 1hr; 2=between 1 and 4 hrs;3= between 4 hrs and one day; 4=more than one day. Distance: 1=less then 30 min; 2=between 30 min and 1hr; 3=between one and two hrs; 4=more than 2 hrs.
Specification Controls (x): poverty rate; illiteracy rate; type of facility where last treatment was received. Exit: distance to hospital; presence of private hospital in the municipality. Voice: voter turnout; number of OTBs; how active are OTBs. Management Rules: frequency of personnel evaluation.
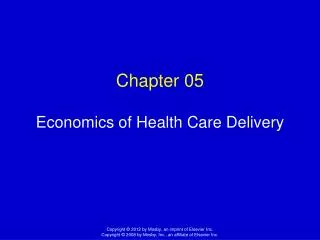
Basic Specification (Table 3) Dependent variable is perception of corruption index (1=never corrupt; 4=always corrupt). Robust t statistics in parentheses.*significant at 5%; significant at 10%.
Extended specification (Table 4) Dependent variable is perception of corruption index (1=never corrupt; 4=always corrupt). Robust t statistics in parentheses. * significant at 5%; ** significant at 1%. Estimation includes a constant (non reported).
Conclusions • The good news: health services are perceived as significantly less corrupt than the central government, the police, and customs. Moreover, users of Seguro services (basic maternal and infant care) report systematically lower corruption ratings. • However, “free” services may not be so free. Informal payments for services that are supposed to be free are extensive in Bolivia.
What are the policy implications ? • Management practices do seem to matter – in particular, facilities with regular monitoring of staff (in this case, written evaluations) can have payoffs in terms of reducing corruption • Voice can play a role, but the solutions are not straightforward. Several voice factors evidently don’t matter: • Electoral turnout per se • Participation in cultural/ religious associations • Density of OTBs in the municipality. However, corruption is lower in those municipalities where OTBs are regarded by municipal leaders as more active.
In addition, in terms of health sector policies: • Significantly lower perceptions of corruption in health posts (the smallest facilities), suggesting that strengthening this type of provision could also improve accountability to the local communities. • Cannot assume that the mere presence of a private health facility in a municipality is an effective exit option: this is not associated with lower perceived corruption.