Download
1 / 8
80 likes | 259 Vues
Comparison of INSTI vs INSTI. QDMRK SPRING-2. QDMRK Study: raltegravir QD vs BID, with TDF/FTC. Design. Randomisation* 1 : 1 Double-blind. W48. W96. N = 389. > 18 years ARV-naïve HIV RNA > 5,000 c/mL Any CD4 cell count No resistance to TDF or FTC. N = 386.

E N D
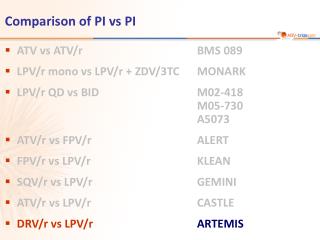
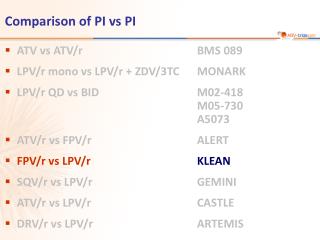
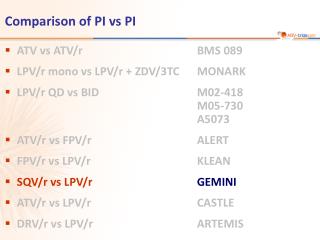
Comparison of INSTI vs INSTI • QDMRK • SPRING-2
QDMRK Study: raltegravir QD vs BID, with TDF/FTC • Design Randomisation* 1 : 1 Double-blind W48 W96 N = 389 > 18 years ARV-naïve HIV RNA > 5,000 c/mL Any CD4 cell count No resistance to TDF or FTC N = 386 *Randomisation was stratified by baseline HIV RNA (< or > 100,000 c/mL) and viral hepatitis co-infection status • Objective • Non inferiority of RAL QD: % HIV RNA < 50 c/mL by ITT, NC=F (lower margin of the 2-sided 95% CI for the difference = - 10%, 90% power) Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
QDMRK Study: raltegravir QD vs BID, with TDF/FTC Baseline characteristics and patient disposition Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
RAL BID RAL QD QDMRK Study: raltegravir QD vs BID, with TDF/FTC Response to treatment at week 48 HIV RNA < 50 c/mL HIV RNA < 50 c/mL at W48(NC=failure analysis) by baseline factors % Primary analysis 91.0 100 88.9 86.6 83.2 75 50 25 * 95% CI for the difference = - 8.3 ; 2.7 N = 386 382 377 367 Mean CD4/mm3 increase at W48 (observed-failure analysis): + 196 (RAL BID) vs + 210 (RAL QD) 0 ITT NC = F Per protocol, observed-failure* 95% CI for the difference =( - 10.7 ; -0.8) 95% CI for the difference = (- 9.0 ; 0.2) * Exclusion of discontinuations due to intolerability or reasons unrelated to treatment Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
Safety at W48 QDMRK Study: raltegravir QD vs BID, with TDF/FTC Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
Virologic failure: definition Non-response = never achieved 2 consecutive HIV RNA < 50 c/mL by week 24 or at time of premature study discontinuation or rebound = after an initial response, confirmed HIV RNA > 50 c/mL QDMRK Study: raltegravir QD vs BID, with TDF/FTC * Genotyping was done only in patients with HIV RNA > 400 c/mL 2/2 (RAL BID) and 7/9 (RAL QD) patients who had emergence of RAL resistance had baseline HIV RNA > 100 000 c/mL Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
QDMRK Study: raltegravir QD vs BID, with TDF/FTC • Pharmacokinetic Data • Trough raltegravir concentrations were more than six times higher with twice-daily dosing than they were with once-daily dosing • Although an association between trough RAL concentrations and efficacy was evident in the once-daily group, no clear threshold could be identified Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK
Conclusion At 48 weeks of treatment, RAL QD was not non-inferior to RAL BID, in combination with TDF/FTC Virologic failure was more common with once-daily dosing especiallyin patients with baseline HIV RNA > 100 000 c/mL More patients in the once-daily group than in the twice-daily group had resistance emergence to both RAL and FTC at the time of virological failure Patients in the once-daily group with low pharmacokinetic values and high baseline viral loads were at particular risk of treatment failure Despite a high response rate, RAL at 800 mg QD cannot be recommended in place of twice-daily dosing for first-line antiretroviral therapy QDMRK Study: raltegravir QD vs BID, with TDF/FTC Eron JJ, Lancet Infect Dis 2011;11:907-15 QDMRK