Download
1 / 34
340 likes | 445 Vues
Explore the crucial role of the innate immune system in fighting infections and its impact on treatment outcomes. Learn about therapeutical advancements and the relevance in different populations, from bone marrow transplant patients to HIV-infected individuals. Dive into the mechanisms of cellular and humoral immunity, including crucial factors like Mannose-binding lectin and MBL deficiency. Uncover the connection between specific MBL haplotypes and susceptibility to bacterial and fungal infections. Delve into research on MBL deficiency and its association with recurrent infections. Discover how MBL levels influence the severity of infections, such as bacterial septic shock.

E N D
Innate Immunity: The First Line Against Infections Juan Pablo Horcajada. Unidad de Enfermedades Infecciosas Hospital Universitario Marqués de Valdecilla Santander. Spain.
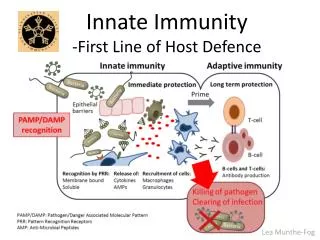
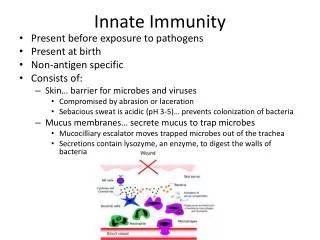
Relevance • In adults there are important differences in • susceptibility to infections • outcome of infections under treatment • Innate immune system is the “third column” of the immun system • There are new therapeutical possibilities
Innate immunity Cellular Immunity Humoral Inmunity
Index • The innate immune system • Mannose-binding lectin • MBL deficiency and infections: susceptibility and severity • Special populations: • Bone marrow transplant patients • HIV-infected patients
Humoral response Cellular response Antibodies Lymphocytes Immunity Innate Adaptative Non-specific Does not generate memory Specific Generates memory Humoral factors Cells External barriers Complement Acute phase proteins Neutrophils Monocytes NK Cells
CLASSIC PATHWAY Ag-Ab Complexes THE COMPLEMENT SYSTEM MBL PATHWAY Microbial surfaces ALTERNATIVE PATHWAY Microbial surfaces MBL-MASP2 MBL-MASP1 C3b C1q C1r C1s C4 C2 C3 C4b C2a C3a, C5a C3b C5b-C9 Inflamation, fagocyte recruitment Membrane attack complex, pathogen lysis Opsonization, elimination of immunocomplexes
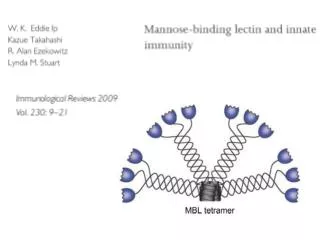
MBL TETRAMER Disulfur bond Proteases (masp) N-terminal Activation C’ collagen first region collagen second region DRC hexose Bacterial surface
Structure of MBL polipeptidic chain D Carbohidrate Recognition Domain (CRD) C Alpha helix region. Interacts with CRD and determines its spatial orientation Collagen region. Functions: fagocytosis, opsonization and protease binding for complement activation B Terminal NH2 segment. Oligomerization through N-terminal cisteins by disulfur bonds A
MBL gen polymorphisms Promotor Exon 1
Serum MBL levels related with different haplotipes High (>1000 ng/ml) HYPA LYQA LYPA Homozygous Sufficient Medium (500-1000 ng/ml) HYPA LYQA LYPA LXPA Heterozygous sufficient Low (200-500 ng/ml) HYPD LYQC LYPB HYPA LYQA LYPA Heterozygous Sufficient-insufficient Very Low (<200 ng/ml) HYPD LYPB LYQC LXPA Homozygous insufficient
MBL levels in relation with haplotypes Homozygous defficient
MBL binding to different microorganisms +++ Candida Aspergillus S. aureus S. pyogenes Bifidobacterium Veillonella ++ E. coli Klebsiella Haemophilus influenza B + S. agalactiae S. pneumoniae S. epidermidis Pseudomonas Enterococcus Clostridium Bacterioides
MBL defficiency and susceptibility to bacterial infections Meningococcal Infection Frequency of homozigous MBL-variants alleles in hospitalized patients 7,7% vs. 1,5% in non-infectious controls OR 6,5 p = 0.0006 Frequency in general population: 8,3% vs. 2,3% in healthy controls OR 4,5 p = 0.06 Hibberd ML. Lancet 1999;353:1049
MBL defficiency and susceptibility to bacterial infections Pneumococal infection Defficient homozygous Controls OR p 28/229 (12%) 18/353 (5%) 2,59 0.002 11/108 (10%) 36/679 (5%) --- 0.046 Roy S. Lancet. 2002;360:1176.
MBL levels in elective abdominal surgery and incidence of bacterial infections N=172 patients N infections: 10 (0,58%) M. Siassi. Biochem Soc Tras 2003;31:774
MBL defficiency associated with recurrent bacterial infections Gomi K. Chest 2004; 126:95–99
MBL defficiency and susceptibility to fungal infections Recurrent vaginal candidiasis Babula CID 2003 Sep 1;37(5):733
MBL defficiency and susceptibility to fungal infections Chronic necrotizing pulmonary Aspergillosis Defficients Haplotypes In Controls p in CNPA 7/10 (70%) 20/82 (25%) 0,004 Crosdale JID 2001
Bacteraemic Pyelonephritis N = 27 Non Bacteraemic Pyelonephritis N = 35 MBL defficiency and severity of infections Low MBL (n=13) 9 (33.3) 4 (11.4) Normal MBL (n=49) 18 (67.6) 31 (88.6) P=0.0362 test Smithson A. 2005 ECCMID . P-1824
Pyelonephritis with septic shock N = 7 Pyelonephritis without septic shock N = 55 MBL defficiency and severity of infections Low MBL (n=13) 4 (57) 9 (16.3) Normal MBL (n=49) 3 (43) 46 (83.7) P=0.030 Fisher exact test Smithson A. 2005 ECCMID . P-1824
Innate immunity Cellular Immunity Humoral Inmunity
MBL Serum levels and Susceptibility to opportunistic Infections in bone marrow transplant patients Prospective study (feb-oct 2005) BMT and infections Follow-up 6 months Periodic MBL serum levels determinations • RESULTS • 12 (50%) autologous and 12 (50%) alogenic. • 55% of infectious episodes: during neutropenic period. • 63% bacterial; 26% viral, 9% fungal • 6 (25%) died because an infectious complication
MBL<1000 * infeccion viral Crosstabulation Count infeccion viral n0 si Total MBL<1000 no 4 6 10 si 10 8 2 Total 12 8 20 P = 0,16 MBL<1000 *gram positive inf Crosstabulation Count gram positive infection no yes Total MBL<1000 no 8 3 11 si 7 2 9 P = 1 Total 15 5 20 MBL<1000 * gram negative infec Crosstabulation Count gram negative infection no yes Total MBL<1000 no 4 7 11 si 3 6 9 P = 1 Total 7 13 20 P = 0.16
MBL<1000 fungal infection no/yes Crosstabulation Count fungal infection no/yes no yes Total MBL<1000 no 11 11 si 6 3 9 P = 0,07 Total 17 3 20 Maximum MBL serum levels ng/mL • Confirmed fungal infection • -Pulmonary Aspergilosis • Pulmonary Mucormicosis • Systemic Candidiasis
Polymorphisms of the Mannose-Binding Lectin Gen and Susceptibility to Opportunistic Infections in HIV-Infected Patients A/A or A/0 n=151 460 (304) 48831 (154112) 0/0 n=39 527 (252) 36579 (152237) p 0.21 0.66 Genotypes CD4 count, mean (SD) Viral load, mean (SD) JP Horcajada et al. ICAAC 2004
S. pneumoniae p 0.65 1 0.28 A/A or A/0 n=151 32 (21) 5 (3.3) 17 (11) 0/0 n=39 7 (18) 1 (2.5) 7 (18) Genotypes Pneumococcal bacteremia Recurrent pneumococcal bacteremia Recurrent pneumonia JP Horcajada et al. ICAAC 2004
Candidiasis p 1 1 1 0.96 A/A or A/0 n=151 7 (4.6) 18 (12) 4 (2.6) 29 (19.2) 0/0 n=39 1 (2.5) 5 (13) 1 (2.5) 7 (18) Genotypes Oral (Muget), n(%) Esophageal, n(%) Vaginal, n(%) Any candidiasis, n(%) JP Horcajada et al. ICAAC 2004
Virus p 0.20 0.15 0.03 0.50 0.58 A/A or A/0 n=151 7 (4.6) 32 (21) 5 (3.3) 2 (1.3) 4 (2.6) 0/0 n=39 1 (2.5) 4 (10.2) 5 (13) 1 (2.5) 0 Genotypes Cytomegalovirus Herpes Zoster Recurrent Herpes simplex Progressive multifocal leukencephalopathy Molluscum contagiosum JP Horcajada et al. ICAAC 2004
Other OI p 1 0.52 0.50 0.10 0.73 1 A/A or A/0 n=151 6 (3.9) 10 (6.6) 2 (1.3) 3 (1.9) 13 (8.6) 1 (0.6) 0/0 n=39 1 (2.5) 3 (7.7) 1 (2.5) 3 (7.7) 2 (5.1) 0 Genotypes Toxoplasmosis Pneumocystis carinii MAI Hairy leukoplakia Condiloma Non-TB Mycobacteria JP Horcajada et al. ICAAC 2004
Tuberculosis p 0.20 1 1 0.35 0.048 A/A or A/0 n=151 15 (10) 3 (1.9) 1 (0.6) 8 (5.3) 27 (18) 0/0 n=39 1 (2.5) 1 (2.5) 0 0 2 (5.1) Genotypes Pulmonary, n(%) Lymph node, n(%) Bone, n(%) Milliary, n(%) Any TB, n(%) JP Horcajada et al. ICAAC 2004
Conclusions (I) • MBL is a key protein of the innate immune system • MBL serum level is genetically determined • Genetic polymorphisms are very prevalent • There is a higher predisposition for some infections in MBL-deficient patients
Conclusions (II) • MBL defficiency is associated with higher severity of infections • In bone marrow transplant MBL deficiency is associated with a higher incidence of invasive fungal infections. • No relation between low MBL levels and the incindence bacterial / viral infections and in these patients
Conclusions (III) • In HIV-infected patients MBL deficiency is associated with a higher incidence of recurrent herpes. On the contrary, tuberculosis is more frequent in patients With normal or high MBL levels. • Milliary tuberculosis is not detected in MBL-deficient HIV-infected patients.