Download
1 / 15
150 likes | 755 Vues
Hospital-Wide Restraint Initiative. Committee Members. Vickie Geha Cathy Klotz Barb Kvale Deb Hanson. Cathy Benninghoff Kathy Boyk Caryn Flournoy Kerri Rahman Ad hoc member: Deana Sievert. Plan – Current Situation.

E N D
Committee Members Vickie Geha Cathy Klotz Barb Kvale Deb Hanson • Cathy Benninghoff • Kathy Boyk • Caryn Flournoy • Kerri Rahman Ad hoc member: • Deana Sievert
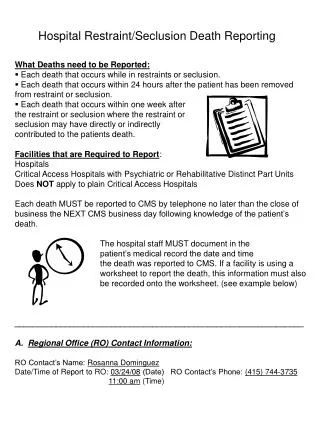
Plan – Current Situation • Many different accreditation bodies have developed standards around the use of restraints. Most have to do with restraint reduction – following the philosophy that inappropriate restraint use could result in patient harm, including death • The FDA now estimates that approximately 100 deaths per year are from restraint use
Plan – Improvement Goal • Reduce restraint use against external benchmark throughout the hospital • Use of external benchmarks as available • Increase staff awareness regarding the standards, use of least restrictive alternatives, and the goals of restraint reduction • Improve documentation of restraint use
Benchmarks • Med/surg benchmark - 3.4 • Rehab benchmark - 3.4 • ICU benchmark - 24.3 • Continue with internal benchmarks for psychiatric units
Plan – Opportunity Statement • Meet compliance regarding documentation of restraint/seclusion use • Maintain or decrease restraint/seclusion in all hospital areas as reasonable • Meet all compliance standards for restraint/seclusion use
Measure - Indicator • Various indicators were used • M/S: number of restraint episodes (any time an order is written) ÷ number of patient days x 100 • MCCU/Rehab: number of hours in restraints ÷ number of patient hours x 100 • Child Psych: number of hours in seclusion/restraints ÷ number of patient days x 100 • Geri-Psych: number of hours in seclusion/restraints ÷ number of patient days/24 hours x 1000 • Documentation indicators
Analyze - Results • Geripsych is almost 100% restraint free • Kobacker continues to make program changes to become restraint free • Increased awareness of staff in the use of restraints • There has been some improvement in documentation, but 90% compliance is not met
Actions • Purchased least restrictive devices such as lap buddies, chair alarms, Velcro waist wrap, activity aprons, wedge cushions, and side-rail protectors • Continue with the Family Sitter Program • Use of 1:1 • Added new committee members • Integrated restraint education in hospital orientation • Revised the documentation tool to include all required elements
Actions • Added the use of freedom splints in the ICUs • Changed to using an external benchmark • Presented to the Med/Surgical Zone yearly • Independent study program offered (contact hours provided) • Presented poster presentations • Recognized staff nurses who documented thoroughly • Counseling staff for documentation issues
Actions • Restraint care plan revised • Recognized 5CD for achieving nursing documentation standards above 90% for one month • Documentation tool revised • Kobacker PI project won first place at the PI fair • Develop 1:1 policy • Develop 1:1 Standards of Care • Continue to have ACs review restraint documentation
Actions – Future Steps • Education of physicians will occur in the area of order writing • Slice/dice data further • Continue to look for patterns • Identify opportunities by population or unit • Continuing to educate at the new employee orientation and nursing orientation
Actions – Future Steps • Independent studies are available • Include restraint education in skills labs • Continue to monitor documentation compliance regarding the many required documentation elements • Make some revisions to the current charting tools to streamline, including the physician order form
Response • Restraint use as it relates to PI is complex, challenging, and often, slow moving • Data collection is time-consuming and labor intensive • Goals must be well defined and the team must celebrate even small successes • Value and perception regarding restraint use varies, but most staff do not think about restraint use the same as a form of treatment
Response • When you think you have the rules down – they change • PI around restraint use is here to stay • It is possible to achieve perfection with efforts from all • Have to keep up with the monitoring to achieve perfection