Download
1 / 29
290 likes | 504 Vues
EVENT HISTORY CALENDARS: AN INNOVATION IN ADOLESCENT RISK BEHAVIOR ASSESSMENT AND COMMUNICATION. Kristy K. Martyn, PhD, RN, CPNP-PC Cynthia Darling-Fisher, PhD, RN, FNP-BC Michelle Pardee, DNP, RN, FNP-BC David Ronis, PhD Irene Felicetti, MS Melissa Saftner, PhD, RN, CNM.

E N D
EVENT HISTORY CALENDARS: AN INNOVATION IN ADOLESCENT RISK BEHAVIOR ASSESSMENT AND COMMUNICATION Kristy K. Martyn, PhD, RN, CPNP-PC Cynthia Darling-Fisher, PhD, RN, FNP-BC Michelle Pardee, DNP, RN, FNP-BC David Ronis, PhD Irene Felicetti, MS Melissa Saftner, PhD, RN, CNM
Related Publication & Research Support • Martyn, K.K., Darling-Fisher, C., Pardee, M., Ronis, D.L., Felicetti, I.L., &Saftner, M.A. (2011). Improving sexual risk communication with adolescents using event history calendars. Journal of School Nursing. Access: http://jsn.sagepub.com/. doi:10.1177/1059840511426577 • We gratefully acknowledge the following grant support by the National Institutes of Health and National Institute of Nursing Research, The Michigan Center for Health Intervention, P30 NR009000.
Theoretical & Evidence Frame • Autobiographical memory (past experiences cues to remembering) (Belli, 1998; Conway, 1996) • Quantitative research (Freedman et al., 1988; Furstenburg et al., 1987; Yoshihama, 2000;Youngblut et al., 1999; 2001) • Clinical assessment (Caspi et al., 1996) • Qualitative research (Martyn et al., 2001; 2002; 2003; 2006; 2009; 2011; 2012) • Interaction Model of Client Health Behavior
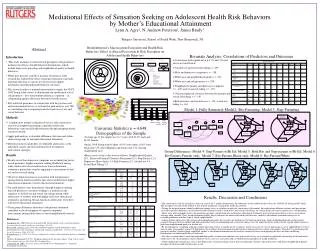
Individual Characteristics Patient-Provider Communication Health Outcomes • Background Variables • Race/Ethnicity, SES,Education, Gender • Social Factors • Previous Risk Behaviors • Communication Process • Affective Support • Health Information • Decisional Control Sexual Risk Behaviors and Intentions • Cognitive Appraisal • Risk Perception • Attitudes Interaction Model of Client Health Behavior: Adolescent Sexual Risk Behavior (Cox, 1982; 2003)
Event History Calendars“My whole life on paper” • Time and context-linked health history graph • Open-ended questions about events, behaviors, relationships and related goals • Shows interrelationships, patterns, triggers • Facilitates patient-provider awareness and communication • Actively engages patients in co-constructing health
Adolescents on Why a Clinical EHC • “[The calendar] would be good to have and fill out, I think. Like if you're at a doctor, I'm sure your doctor would need to know something about you. And half of this is definitely not on my record. My whole life on paper.”
Specific Aims • Specific Aim 1: To examine the effects of the EHC intervention on adolescent risk perception, communication with provider, and intentions to abstain from intercourse and avoid unprotected intercourse post-intervention and at 1- and 3-months.
Specific Aims • Specific Aim 2: To explore whether the EHC intervention is viewed by adolescents and providers as easy to use and helpful for reporting and discussing sexual histories.
Methods • Mixed method exploratory study • Pilot intervention study • Thirty 15-19 year old females and males • Two nurse practitioners • School-linked Health Center in SE Michigan
Methods • Adolescents self-administered the Event History Calendar (EHC), discussed their EHC with a nurse practitioner during a clinic visit, completed pre, post, 1 and 3-month surveys, a post-intervention interview • The nurse practitioners completed post-intervention surveys and a post-study interview • Adolescent received $25 gift cards after each session
EHC Intervention Adolescent self-administers the EHC using open-ended questions on context and risk behaviors, autobiographical memory cues, and retrieval cycles • Encourages reflection (i.e., cognitive appraisal) on their time-linked integrated sexual risk history graph • Prepares the adolescent to discuss his or her actual and potential risk behavior history with the provider
EHC Intervention – Pre-Visit • Prior to the visit with the adolescent, the provider reviews the adolescent’s EHC in context of a timeline that shows interaction of risk behaviors and life events • Provider identifies potential risks and strengths in context
EHC Intervention Visit • Provider and adolescent sit side-by-side and together view and discuss the adolescent’s integrated sexual risk history, facilitating cognitive appraisal, affective support, decisional control • Meaningful (i.e., tailored) adolescent-provider communication
Adolescent Surveys • Clinic Visit: • Adolescent Pre-EHC Survey: Demographics, Risk Behavior, Attitudes, Intentions, Risk Perception, and Adolescent-Provider Communication • Adolescent Post-EHC Visit Survey: Repeated above measures • One- and Three-Month Sessions: • Adolescent Outcomes Surveys: Risk Behavior, Attitudes, Intentions, and Risk Perception • Alphas = .61-.99 & Positive feedback
Provider Data • Clinic Visit: • Provider Post-Training Survey: Demographics, Provider-Adolescent Communication (Usual) • Provider Post-Visit Survey: Provider-Adolescent Communication (This Visit); Perceptions of Clinical Use of EHC • End of Study: • Provider Post-Study Survey • Interview • Chart Audit
Adolescent Demographics • Participants School-linked Health Center patients • Mean age: 17.3 years; Age Range: 15-19 years • Study Retention over 3 months (95.5%)
Comparison of Sexual Risk Behavior – Study Sample and Detroit YRBSS
Survey Results Adolescent-Provider Communication (Pre- & Post-Visit) • Greater Satisfaction with Communication (p=.004) • Greater Satisfaction with Interpersonal Style (p=.001) • Greater Involvement in Decision-Making (p=.001) • Greater Amount of Communication (p<.001) about • Sexual Activity • Risk Behaviors • Risk Patterns Over Time • Linkages Between Risk Behaviors
Survey Results Risk Behavior (Pre-, Post-Visit, 1 & 3 months) • Decreased sexual intercourse at one month (p=.031) • Sex in last 30 days (97%, 100%, 79%, 88%) • Condom use last sex (57%, 54%, 48%, 59%)
Comparison of Sexual Risk Behavior1 & 3 Month Post-Intervention
Adolescents’ Perception of the EHC and Provider Communication • “It’s not like I had to bring it up” • Getting communication started • “Seeing it for my own eyes” • Increasing awareness of risks • “Just getting it all out there” • Encouraging discussion about sexual risks • “Made me express myself more” • Enhanced communication with provider
Providers’ Perception of the EHC and Adolescent Communication • “[The EHC] was very easy to show [the adolescent] visually what their behavior was.” • “I think we got a richer amount of information and were able to . . . intervene on a different level.” • “I think they enjoyed filling it out . . . allowed them to look at their behavior in a way that they haven’t in the past.”
Conclusions • The Event History Calendar (EHC) can easily be integrated with tools and practices in health care settings to actively engage patients in risk assessment and communication with providers.
Eliciting Patient-Desired Outcomes • “My future goals” • “I liked the calendar . . . I haven’t really sat down and rethought back in my past. But it really made me sit down and think about who was I with, what was I doing, and what are my goals.”
Conclusions • EHC methods enhance person-centered health care and research by eliciting and including patient-desired outcomes • in health research • in health care decision-making • with patients of variety of ages, cultures, health needs
EVENT HISTORY CALENDARS: AN INNOVATION IN ADOLESCENT RISK BEHAVIOR ASSESSMENT AND COMMUNICATION Kristy K. Martyn, PhD, RN, CPNP-PC Cynthia Darling-Fisher, PhD, RN, FNP-BC Michelle Pardee, DNP, RN, FNP-BC David Ronis, PhD Irene Felicetti, MS Melissa Saftner, PhD, RN, CNM