Download
1 / 25
250 likes | 433 Vues
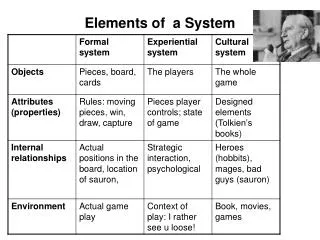
Elements of Health System Financing Lecture 4 of 6. Paying Medical Personnel (mainly in community) . Objectives and Structure of Today ’ s Lecture. Revisit the concept of “ Payment ” vis a vis ‘ Allocation ” Institutional frameworks

E N D
Elements of Health System FinancingLecture 4 of 6 Chernichovsky Draft
Paying Medical Personnel (mainly in community) Chernichovsky Draft
Objectives and Structure of Today’s Lecture • Revisit the concept of “Payment”vis a vis‘Allocation” • Institutional frameworks • Delineate the basic payment options for community providers • Discuss how well each option serves different aims of the health system. Chernichovsky Draft
Part A: Review and Introduction Chernichovsky Draft
“Contracting” vs. “Purchasing” • “Contracting” (akin to ‘allocation’) • Paying an ‘intermediary’ -- not necessarily the provider -- for organizing and managing the consumption (OMCC) a specified package of care. Relates to the concept of ‘budget holding’ • “Purchasing” (akin to ‘procuring’ care) • Paying a provider for actual provision of care • The splits can be fuzzy • Some OMCCs are providers: HMOs and sickness fund who provide care • Some providers are OMCCs: British and other budget holding MDs. Chernichovsky Draft
Part B: Institutional Arrangements Chernichovsky Draft
Contracting / Allocation Scheme Chernichovsky Draft
Potential Flows of Funds or Allocation Arrangements Chernichovsky Draft
Basic Models for OMCC/Contracting Institutions Chernichovsky Draft
Basic Models for OMCC/Contracting Institutions Chernichovsky Draft
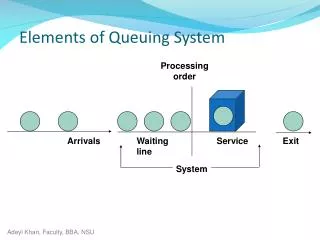
Provider Institutional Framework • Primary care clinics in the community • Preventive care clinics • Curative care clinics • Specialized-professional clinics • Hospitals • Outpatient care • In-patient care • Others • pharmacies • labs and other support facilities Chernichovsky Draft
Provider Institutional Framework:Focus today • Primary care clinics in the community • Preventive care clinics • Curative care clinics • Specialized-professional clinics • Hospitals • Outpatient care • In-patient care • Others • pharmacies • labs and other support facilities Chernichovsky Draft
Part C: Payment Options Chernichovsky Draft
Payments to Providers • The incentive system • Influences: • Attitude to patients • Quantity and quality of service and care Chernichovsky Draft
The Basic Matrix: Health System Aims Vs. Financing Elements, Not Including “Level” and “Health”) Chernichovsky Draft
Basic Options to Pay Providers in the Community • Fee-for-service (FFS) • FFS with global capping • Capitation, with fund holding • Wages • Combinations Chernichovsky Draft
Associations Between Pay Methods apitation FFS Capped FFS Capitation Wages (Prospective) (Retrospective) Chernichovsky Draft
Criteria for Ranking Options vis a vis Health System Aims • Equity • Provider willingness to reach out to the patient and his or her needs. Higher ranking to quantity of patients rather than better quality to each. (Universality principle.) • Macro-economic efficiency and cost containment • Ability of provider to inflate /push aggregate cost of care • Micro-economic efficiency • Provider willingness of to save on overall resources • Client satisfaction • Provider willingness to reach out to the patient with at least quality of services (as opposed to quality if care) Chernichovsky Draft
Potential Impact on Equity –(Ordinal Ranking) Chernichovsky Draft
Potential Impact on Macro-economic Efficiency (Ordinal Ranking) Chernichovsky Draft
Potential Impact on Micro-economic Efficiency(Ordinal Ranking) Chernichovsky Draft
Potential Impact on Client Satisfaction(Ordinal Ranking) Chernichovsky Draft
Part D: Summary Chernichovsky Draft
Goals Pay Mechanism Horizontal Equity (through universality) Macro- Economic Efficiency (through cost control) Production Efficiency Client Satisfaction from Service Fee-for-service 3 1 2 4 Fee-for-service with a global capping* 2–3 4 3 3 Capitation with fund holding 4 (Highest) 2-3 4 2 Wages 1 (Lowest) 2-3 1 1 Provider Payment Options vs. System Aims - Summary Chernichovsky Draft
What next? Pay for hospitalization. Chernichovsky Draft