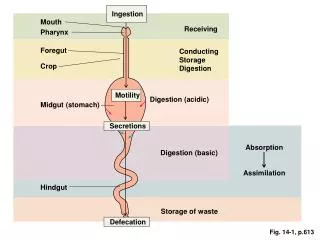
Ocular Motility II
Ocular Motility II. Kenn Freedman M.D. Supranuclear Cranial Nerves Extra-ocular Muscles. Older woman with diabetes suffered sudden onset of Right IIIrd nerve palsy, left elevation defect and left sided weakness. Oculomotor Nerve. Complex Nucleus in Midbrain


Ocular Motility II
E N D
Presentation Transcript
Ocular Motility II Kenn Freedman M.D.
Older woman with diabetes suffered sudden onset of Right IIIrd nerve palsy, left elevation defect and left sided weakness
Oculomotor Nerve • Complex Nucleus in Midbrain • Exits interpeduncular space passing several vessels including PCA • Cavernous sinus • Superior Orbital Fissure • Superior and Inferior Divisions • Superior: Levator and SR • Inferior: MR, IR, IO
Third Nerve Palsy • Aneurysm • Microvascular – DM, HTN, heart disease • Trauma • Neoplasm • Syphilis • Other, Undetermined
Third nerve palsy Microvascular
Young woman presented with left sided headache and drooping of her eyelid
Patient could not move her eye up, down or toward her nose, but she could abduct. Her pupil on the left was much larger than the right.
Brainstem Syndromes • Weber’s - ipsalateral pupil involved IIIrd - contalateral hemiplegia - fasicle of IIIrd Nerve where traverses cerebral peduncle • Benedikt’s – ipsalateral pupil involved IIIrd - contralateral limb intention tremor, hypokinesia and ataxia - Fasicle of IIIrd nerve as it traverses the red nucleus
Management of Third Nerve Palsy • When to do neuro-imaging and/or arteriogram? • Important factors: PAIN, PUPIL, PROGRESSION Other Possible testing: CBC, ESR, BS
In general You get imaging on PUPIL INVOLVED Third nerve palsies
Relative Pupil Sparing0.5mm <Anisocoria < 2mm(Larger pupil still RTL) • Out of 24 patients: • 10 - had compressive lesions! • 10 - “infarction” • 4 - other Neurology 2001; 56: 797
Imaging Options • MRI • MRA – no contrast • Cerebral Arteriogram – some risk
Management Isolated Third Nerve Palsy If patient is diabetic/ hypertensive and the pupil is not involved and they do not have too much pain*, then it would be reasonable to follow them up without imaging studies, depending on your comfort level. You should see some resolution of a microvascular palsy in at least two months.
Aberrant Regeneration • One of many possible findings due to misdirection of axon fibers as healing occurs • Lid retraction on downgaze • Lid elevation or pupil constriction with attempted adduction • Globe retraction with attempted upgaze or downgaze • Others also possible
Lid Lag on Downgaze • Congenital Ptosis -Levator Maldevelopment • Graves Ophthalmopathy • Surgery, Trauma • Aberrant Regeneration of 3rd -pseudo von Graefe’s phenomenum
Primary Aberrant Regeneration? • Motility problems like those described above without an acute third nerve palsy preceding them. • Suggestive of a cavernous sinus mass
Trochlear Nerve • Superior Oblique • Long course of nerve from posterior midbrain to orbit Midbrain
4th Nerve Palsy • Diplopia –usually vertical • Sometimes Cyclo-diplopia • Head tilt and/or turn • Diplopia can worse or better on downgaze • Findings can evolve over time
Fourth Nerve Palsy • Hypertropia • Overaction of Ipsalateral Inferior Oblique Muscle • Underaction of SO not often obvious • Excyclotorsion • Incommitant
Fourth Cranial Nerve PalsyIncommitance • Hypertropia • Hypertropia worse on contraleral gaze • Hypertropia worse on ipsalateral head tilt • E.g. “right – left - right” • or “left - right – left”
Right- Left- Right 15 RHT 3 RHT 2 RHT 7 RHT 18 RHT
Three Step Test is only valid for Neurologic and not mechanical muscle problems Assumes only one paretic muscle
Excylotorsion • With red maddox rod over Right and white over Left Shows a right excylcotorsion consistent with a right SO palsy
Fourth Nerve Palsy • Congenital* • Traumatic • Microvascular • Neoplasm • Aneurysm – not common • Other * Congenital – often decompensate later in life with “sudden” onset of diplopia, will have large vertical fusional amplitudes
Fourth Nerve Palsy(Traumatic) Upshoot in adduction characteristic of Overaction of left inferior oblique
Upshoot in Adduction • Most Commonly IOOA • DVD • Duane’s Syndrome
Bilateral Fourth Nerve Palsy • Alternating Hypertropia e.g. LHT in right gaze RHT in left gaze • Large Excyclotorsion >10-15 degrees • V pattern
Vertical Misalignment • Fourth Nerve Palsy • Graves Disease • Post-operative muscle problem • Skew Deviation • Third Nerve Palsy –inferior or superior division • Brown’s Syndrome • Other Orbital Disease • Plus More
Management of Isolated Fourth Nerve Palsy • Usually no work up necessary as most cases are traumatic or congenital. If no history of trauma or signs of congenital palsy then : • Does patient have vasculopathic risk factors? • Yes: Observe • No: Medical evaluation, maybe image
Abduction Deficit New onset diplopia Patient asked to look To the left
Abduction Deficit • Sixth Cranial Nerve Palsy • Graves Ophthalmopathy • Myasthenia Gravis • Orbital – tumor, inflammatory • Duane’s Syndrome Type I • Medial Wall Fracture • Past LR recession • More!