Download
1 / 55
550 likes | 980 Vues
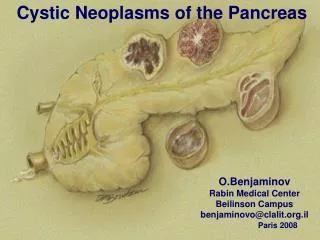
Northern California SGNA Fall Conference 2010 Pancreas Neoplasms. Randall E Lee, MD, FACP Gastroenterologist, VA NCHCS Associate Clinical Professor of Medicine, UC Davis. Disclaimer. No financial conflicts of interest or sponsorships. Pancreas neoplasms.

E N D
Northern California SGNAFall Conference 2010Pancreas Neoplasms Randall E Lee, MD, FACP Gastroenterologist, VA NCHCS Associate Clinical Professor of Medicine, UC Davis
Disclaimer • No financial conflicts of interest or sponsorships
Pancreas neoplasms • Pancreas anatomy, embryology, physiology • Pancreas endocrine neoplasms • Pancreatic adenocarcinoma • Pancreas cystic neoplasms
Pancreas Embryology
Pancreas physiology • Exocrine • Endocrine
Pancreas physiology • Exocrine • Secretion into a duct • Endocrine
Pancreas physiology • Exocrine • Secretion into a duct • Endocrine • Secretion directly into the bloodstream
Pancreas structure • Acini • Islets
Pancreas structure • Acini • Connected to ducts • Exocrine function • Islets
Acini • Connected to ducts • Exocrine function • “acinarization” • Islets
Pancreas structure • Acini • Islets • Not connected to ducts • Endocrine function
Pancreas structure • Acini • Connected to ducts • Exocrine function • “acinarization” • Islets • Not connected to ducts • Endocrine function
Pancreas physiology • Exocrine • Amylase: carbohydrate • Lipases: fat • Proteases: protein • Endocrine
Pancreas physiology • Exocrine • Amylase: carbohydrate • Lipases: fat • Proteases: protein • Endocrine
Pancreas physiology • Exocrine • Endocrine • Insulin (beta cells) • Glucagon (alpha cells) • Pancreatic polypeptide (PP cells) • Somatostatin (D cells)
Pancreatic endocrine neoplasms • Insulinoma • Gastrinoma • Glucagonoma • VIPoma
Pancreas endocrine neoplasms • Insulinoma • hypoglycemia • Gastrinoma • Glucagonoma • VIPoma
Pancreas endocrine neoplasms • Insulinoma • Gastrinoma • “Zollinger-Ellison Syndrome” • Peptic ulcer, GERD, diarrhea • Gastrin is not normally produced in the pancreas! • Glucagonoma • VIPoma
Pancreas endocrine neoplasms • Insulinoma • Gastrinoma • Glucagonoma • Hyperglycemia • Weight loss • Rash • VIPoma
Glucagonoma rash: Necrolytic migratory erythema
Pancreas endocrine neoplasms • Insulinoma • Gastrinoma • Glucagonoma • VIPoma • Severe diarrhea • Hypokalemia • Volume depletion
Pancreatic endocrine neoplasm localization: CT SR scintigraphy “Octreoscan” EUS
Pancreas endocrine neoplasm: treatment • Medical suppression of symptoms • Surgical resection
Pancreas adenocarcinoma • Usually arises from the duct • Men more than women, older than 45 years • Generally poor long-term prognosis • No good screening / early detection methods
Pancreas adenocarcinoma: perspective National Cancer Institute, 2010
Pancreas adenocarcinoma: clinical presentation • Location! • Location! • Location!
Pancreas adenocarcinoma: clinical presentation • Symptoms occur late in disease course. • Head of pancreas: • Jaundice • Palpable non-tender gallbladder (Courvoisier’s sign) • Advanced: • Fat malabsorption: steatorrhea • Pain • Fatigue, anorexia, weight loss
Pancreas adenocarcinoma: diagnosis • CT +/- biopsy • MRCP • ERCP & brushing / biopsy • EUS & FNA
ERCP: “Double-duct” sign
Pancreas malignancy: ERCP • Sphincterotomy • Grounding pad, generator, sphincterotome • Strictures • Guidewire(s), dilators, stents • Cytology brush, glass slides, fixative
Pancreas malignancy: EUS • Fine-needle aspiration & biopsy • Coordinate with pathologist • Cytology fixative, glass slides
Pancreas adenocarcinoma: treatment • Curative resection • Palliative therapy
Pancreas adenocarcinoma: survival after Whipple
Pancreas adenocarcinoma: treatment • Curative resection • Palliative therapy
ERCP • cannulation
ERCP • sphincterotomy
Pancreas Adenocarcinoma: survival
Pancreas neoplasms: cystic • Mucinous cystic neoplasms • Serous cystadenomas • IPMNs
Mucinous cystic neoplasm • Cystic tumors filled with mucin • Women > men • Body & tail of pancreas • Always considered premalignant / malignant • Surgical resection
Serous cystadenoma • Cystic tumor filled with serous fluid • Women > men • Body & tail of pancreas • Generally benign, but can cause complications
I P M N