Download
1 / 46
610 likes | 1.09k Vues
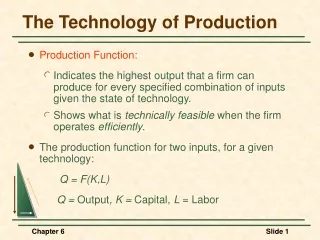
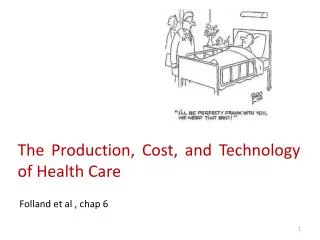
The Production, Cost, and Technology of H ealth C are. Folland et al , chap 6. Outline. Production and the possibilities of substitution Costs in Theory and Practice Technical and allocative inefficiency Technological changes and costs Diffusion of new health care technologies.

E N D
The Production, Cost, and Technology of Health Care Folland et al , chap 6
Outline Production and the possibilities of substitution Costs in Theory and Practice Technical and allocative inefficiency Technological changes and costs Diffusion of new health care technologies
Production and the possibilities of substitution Economist often note that different techniques are available to produce the same product. A single technique is one recipe for production, meaning one specific combination of inputs Economists describe production of output as a function of labor and capital When multiple techniques are available, one can choose a relatively capital-intensive (labor-intensive) technique during times when capital (labor) is relatively cheap. Flexibility: the ability to substituteone input, such as capital, for another input, such as labor, while maintaining the level and quality of output
Q3 C Q2 B Q1 P A N Degree of substitution between physicians and nurses Isoquants where no substitution is possible Physician hours Nurse hours Isoquants show the technological trade-off between nurse hours and physician hours in the production function (treating one patient case in hospitals). Only one sensible production technique combine the two inputs.
What is an isoquant? The set of points at which the same quantity of output is produced while changing the quantities of two or more inputs. While an indifference curve mapping helps to solve the utility-maximizing problem of consumers, the isoquant mapping deals with the cost-minimization problem of producers. Isoquants typically show the technological trade-off between inputs in the production function, and the decreasing marginal returns of both inputs
Degree of substitution between physicians and nurses (cont.) • The isoquants (labelled Q=1, Q=2, Q=3) show the possible combinations of nurse hours and physician hours required to treat 1/2/3 patient cases in hospital • The two inputs are perfect complements; with a level of production Q1, Q2, Q3, nurse hours and physician hours can only be combined efficiently in the certain ratio 0P/0N (that is also the slope of the segment 0M) occurring at the kink in the isoquants.
Degree of substitution between physicians and nurses (cont.) • 0P physician hours are required to produce 1 case and the addition of nursing hours beyond 0N will not add to output unless physician hours also are increased. • The isoquant is flat when moving to the right from M • adding nurses beyond the required combination produces no more output (i.e. they would be wasted) • The isoquant is vertical when moving upward from M Additional physician hours beyond the required ratio combination are simply wasted resources.
The slope of any isoquant is the Marginal Rate of Technical Substitution: The rate at which nurse and physician hours can be exchanged while still maintaining output Physician hours Physician hours 5 4 3 2 Y P 1 R Q3 Q3 1 2 3 4 5 Q2 Q2 Nurse hours Nurse hours N S Q1 Q1 Degree of substitution between physicians and nurses (cont.) Isoquants where substitution is possible The isoquant is a smooth downward-sloping convex curve. It means that many combinations of inputs could be chosen without being wasteful. Each point on the isoquant represents a different technique.
Degree of substitution between physicians and nurses (cont.) • Note that even tough we can substitute, nurses with physicians are not equivalent. A fixed number of nurses cannot always replace a physician. • Moving along the curve from point Y to point Z, the rate of substitution changes the slope becomes flatter (diminishing Marginal Rate of Technical Substitution)
Degree of substitution between physicians and nurses (cont.) • To replace one hour of physician time at point Y requires some number of nursing hours • At point Z where we are using fewer physician hours, we require a much greater number of nursing hours as physician time grows scarcer relative to nursing hours, it becomes more difficult to replace • The curve may even become flat at some point, indicating that we have reached a minimum of required physician time
What degree of substitution is possible? What Does the Research Suggest? The work done by economists suggests that substitution possibilities could be substantial. Depending on the number of physician hours employed, one physician extender1could substitute for 25 percent to more than 50 percent of a physician’s services (Brown, 1988; Deb and Holmes, 1998; Liang and Ogur, 1987; Okunade and Suraratdecha, 1998) 1 Specially trained physician assistants or nurse practitioners who are utilized to perform certain tasks, including some that formerly were performed by physicians
Elasticity of substitution The elasticity of substitution measures the responsiveness of a cost-minimizing firm to changes in relative input prices. Es = 0 No substitutability. Es= 1 Perfect substitutability
Elasticity of substitution (cont.) If a firm, like a hospital, were a cost minimizer, then it would be responsive to changes in input prices, and it would tend to respond by shifting away from the now costlier input to the now relatively cheaper input. Example: if physician salaries increased relative to nurses salaries, then we would observe hospitals substituting nurses for physicians.
Empirical Evidence for Input Substitution in Hospitals Table 6-1 Substitution Elasticities for Teaching and Nonteaching Hospitals Evaluated at the Mean The table shows the estimates of elasticities of substitution between pairs of inputs. Example: a 1% increase in the price of medical staff relative to nurses would result in a 0.547% decrease in the ratio of medical staff to nurses.
Empirical Evidence for Input Substitution in Hospitals (cont.) • “All inputs in both teaching and nonteaching hospitals are substitutes for each other” • It may seem nonsensical that one can substitute people for beds; but beds here represent a convenient measure of the various and complex capital inputs used by a hospital. • Data suggest that even in hospital care production, where labor is the critical input, capital can be substituted on the margin for labor
Costs in theory and practice:Deriving the Cost Function Isoquants show the combinations of inputs to produce a given output Isocost curves (downward sloping) show the combinations of K and L that together cost a given amount. The combination of the production function represented by the isoquants and the cost requirements represented by the isocost curves generates a set of outcomes, (or points C, F, and G in the previous graph). of tangency is the expansion path. It shows the cost-minimizing combinations of capital and labor that can be used to produce 100, 150 and 200 physician office visits, respectively. Figure 6-2 Production Function for a Hypothetical Physician Practice
Cost minimization • Let TC be the level of Total Costs Money can buy many combinations of K and L whose costs add up to: TC = rK + wLISOCOST EQUATION r is the rental price of capital (the cost to the firm of using the capital for one period) w is the wage rate of labor From the isocost equation: K= TC/r – (w/r)*L ISOCOST LINE
Cost minimization(cont.) • The expansion path supplies the information that associates a given output with its minimum cost. • When these costs and output data are recorded in a graph, the result is the firm’s total cost function. Figure 6-2 Production Function for a Hypothetical Physician Practice
Cost minimization: an example A firm wants to produce a output of 100 visits. The least cost production of 100 visits occurs at input combination L=20, K=25 at point C on isocost curve AB. Input prices: r = $1,200 w = $1,000 Output cost of producing 100 visits: $50,000 Output cost of producing 150 visits: $78,000
Economies of Scale • The long run total cost function can be transformed to express information about economies of scale. • The long-runaverage costs for a firm can be calculated by dividing the given cost level by the corresponding number of physician visits. • A firm experiences economies of scale when its long-run average cost is declining as output increases.
Economies of Scale (cont.) Figure 6-3 The Long Run Average Cost • Economies of scale in region AB • Diseconomies of scale in region BC
Economies of Scale (cont.) • Economies of scale (in costs) • Average cost per unit of output falls as the firm increases output. Specialisation of labor and capital → increasing returns to scale in production e.g. If a hospital doubles its number of nurses and beds, it may be able to more than double the number of patients it cares for. - At some point, economies of scale are exhausted, and diseconomies of scale set in. • Diseconomies of scale(in costs) -Average cost per unit of output increases as the firm increases output. When a firm becomes too large →decreasing returns to scale in production e.g. excessive bureaucracy, breakdown in communication flows. - An increase in all inputs results in a less than proportionate increase in output. At this point, the average cost per unit of output rises, and the Long Run Average Cost slopes upwards.
Economies of Scale (cont.) • What output level would a profit-maximizing firm choose in this case? • At point QB its average costs are lowest (ACB) BUT a firm is not in the business of minimizing its average costs and would do so only if, coincidentally, the output that minimized costs also maximized profits.
Economies of scope • Economies of scope occur whenever it is possible to produce a range of goods jointly more cheaply than they can be produced separately. • By definition, economies of scope are possible only for a multiproduct firm and because many health care firms (e.g. hospitals) are multiproduct in nature, the concept is highly relevant • Economies of scope can arise at any point in the production process (acquisition and use of raw materials, distribution, marketing) • Possible sources:
Economies of scope (cont.) • General hospitals can spread the fixed costs of operating rooms and intensive care units over multiple different operations. They can operate at full capacity by treating all types of patients. • Know-how and marketing can be spread over products sharing similar technology • Research and development because the cost and production of developing a drug can be extended to other related drugs.
Economies of scope: an example Suppose that there are two hospitals in town: • pediatric; • geriatric Would the total cost of “geriatric + pediatric care” be lower if one single hospital provided both? E.g. Things learned in pediatrics have applications in geriatrics and the two could support each other so that the result would be lower total costs. If so, by producing the two different outputs jointly, we achieve economies of scope.
Modern Results on Economy of Scale • The most recent research supports claims that economies of scale exist in hospitals. • Preya and Pink (2006) studied costs of Canadian hospitals prior to a massive consolidation, finding “large scale unexploited gains to strategic consolidation in the hospital sector” (p. 1049). • Dranove and Lindrooth (2003) studied a large number of hospital consolidations, they found “significant, robust, and persistent savings for mergers, 2, 3, and 4 years after consolidation” (p. 996). • These results suggest that many hospital mergers might be justified on the basis of cost savings to society
Nice article on the economies of scale and scope http://www.economist.com/node/12446567
Technical and allocative efficiency Efficiency can be measured not only in terms of economies of scale, but also in terms of • technical efficiency: the producer is achieving a maximum output from a given input combination. • allocative efficiency: each firm responds optimally to input prices
Technical efficiency with one input • The production frontier is the production function f(L). • Each firm’s actual experience is indicated by a firm number. • Technical inefficiency results when a firm uses more resources than necessary to produce a given level of output. It is as if workers or machines were misused, not working at full capacity, or not cooperating well • A technically inefficient firm falls off its frontier. Figure 6-5 Technical Efficiency and Inefficiency at the Firm Level. One input.
Technical efficiency with two inputs • The convex curve is an isoquant representing frontier practice treating for 100 cases. • Each firm’s actual experience is indicated by a firm number. • A technically inefficient firm falls off the isoquant.
To measure technical inefficiency How firms inefficiencies are measured? • Relative distances from the frontier: • Output (vertical) distance (what output could have been achieved with this input?) OR • Input (horizontal) distance (how many fewer inputs could have achieved this output)
Allocative efficiency Technical efficiency applies conceptually to production within a given firm. • By contrast, allocative efficiency requires the efficient allocation of inputs between firms and between outputs. It requires that each type of capital and labor be put to its most rewarding use in society. • Allocative efficiency requires that each firm responds optimally to input prices; correspondingly, allocative inefficiency implies choosing an inappropriate combination of inputs in the sense that inputs and their prices have not been appropriately considered.
Allocative efficiency (cont.) • Q = 100 is the isoquant for 100 cases. • Assume that the firm being examined is currently producing its desired level of output, and that the desired level happens to be 100 cases. • Two isocost curves also are depicted, with one indicating a cost level of $50,000 and the other a cost level of $42,000. • Suppose that the firm in question was observed operating at a point A. • Because this firm is treating 100 cases using an input combination on the 100 cases isoquant, we can say this firm is technically efficient. • However, it is not allocatively efficient. At the current input prices, it uses too much capital, and not enough labor.
Allocative efficiency (cont.) • A tangency implies an equality of the ratio of input prices to the ratio of marginal products for the inputs (the equality of marginal output per dollar for each input). • This is the firm’s appropriate response to input prices, and its key condition for allocative efficiency.
Technological changes and costs • The rapid pace of technological change in the health care industry raises economic questions about the effects these changes will have. • Technological change may • reduce costs when it provides less costly production methods for standard “old” products; • increase costs when it improves the quality of care or introduces new and costlier products. • Because it often raises costs in the health sector, many researchers hypothesize technological change to be the major contributor to health sector inflation. • Deep and widespread insurance coverage in the health sector may induce technological innovations of the type that increase costs.
Cost Decreasing Technological Change • Quality of care is constant. • The isoquants represent 100 cases before and after a technological change. • The technological improvement shifts isoquant Q = 100 toward the origin (i.e. same output can be produced with fewer inputs). • The result is a reduction in the costs of producing 100 cases.
Cost Increasing Technological Change • Higher quality of care • The isoquants represent 100 cases before and after a technological change. • The technological improvement shifts isoquant Q = 100 away from the origin (i.e. same output requires more inputs). • The result is an increase in the costs of producing 100 cases. • The typical patient will pay more for care
Health care Price increases when technological change occurs How do we measure the cost of a treatment when the treatment changes radically in one or two decades? • E.g. heart attack treatment (myocardial infarction) changed substantially from 1975 to 1995. • Some new effective inputs proved extremely inexpensive (e.g. aspirin). • Some medical object did not exist in 1975, such as the intraorticballoon pump. • Treatment practices changed; the average length of a hospital stay is now much shorter. • The treatments are now more effective and have improved the length and quality of life for heart attack victims.
Health care Price increases when technological change occurs: Cutler et al. To see whether heart attack treatment in 1995 was more expensive per episode than in 1975, we must hold quality constant within the analysis. Cutler et al. (1999) developed two myocardial infarction treatment price indexes that measure patient gains in quality-adjusted life-years (QALYs). They evaluated these gains in dollar terms, and allowing for errors, particularly in valuing life years, these authors proposed a range of price inflation estimates. Their research shows clearly that 1. technological change makes a difference in patient lives; 2. the fact that substantial quality improvement had previously been omitted meant that previous estimates of inflation in health care needed to be reduced.
Health care Price increases when technological change occurs: Cutler et al. (cont.) Source: Cutler et al (1999) , Price increases of treatment of myocardial infarction (1983-1994) QALYs: quality-adjusted life years. • Technological change improves patient lives • Unadjusted indices show price inflation but quality adjusted indices show price deflation!
Diffusion of new health care technology: Who adopts and why? Two basic principles guide technology adopters: • profit E.g. physicians tend to adopt a new surgical technique if they expect to increase their revenues (enhancing reputation or by improving the well-being of their patients). • information channels Networking effect: Highlight the role of friends, colleagues, journals, and conferences in informing and encouraging the adoption decision
Diffusion of new health care technology: Who adopts and why? (cont.) A firm will tend to adopt an innovation when the present value of future profits due to the innovation is positive. Waiting: Disadvantage: provide competitors with an advantageous share of the market Advantage: learn from future advances and from the experience of others. It may reduce risks so more risk-averse firms may choose to wait somewhat longer.
Classic Pattern of Diffusion:Logistic Function Figure 6-10. The Diffusion of a New Technology • = • where • Pt is is the proportion of individuals or firms adopting by time t • K is the maximum potential proportion of adopters • a and b are parameters to be estimated • The initial stage of growth is approximately exponential, then, as saturation begins, the growth slows and, at maturity, growth stops.
Empirical Findings • Escarce’s(1996) data fit this time pattern quite well. • He studied a new surgical procedure, laparoscopic cholecystectomy, introduced in 1989, which is a minimally invasive technique to remove diseased gall bladders. • He found the diffusion curve to fit the logistic pattern common to diffusion studies.
Empirical Findings (cont.) • Adopting surgeons were more likely to be younger, male, board-certified1, U.S. medical school graduates, and urban-located (Escarce, 1996) . • Younger individuals are more likely adopters. In fact, in one study older physicians proved less likely to adopt even though their expected gains in profit were much higher than for their younger counterparts (Rizzo and Zeckhauser, 1992). • Others suggest that followers are more likely to emulate the “star” physicians, ones with the most impressive credentials (Burke et al., 2007). 1Board certification is the process by which a physician in the United States demonstrates through either written, practical, and/or simulator based testing, a mastery of the basic knowledge and skills that define an area of medical specialization.