POLYCYTHEMIA VERA
POLYCYTHEMIA VERA. EPIDEMIOLOGY. MALE: 2.8 PER 100,000 FEMALE: 1.3 PER 100, 000 Source: Mayo Clinic ( W illiams Hematology7 th ed. 2007) M:F = 3:2 6 th decade of life. ETIOLOGY. Somatic mutation on chromosome 9p which encodes tyrosine kinase -JAK 2

POLYCYTHEMIA VERA
E N D
Presentation Transcript
EPIDEMIOLOGY • MALE: 2.8 PER 100,000 • FEMALE: 1.3 PER 100, 000 • Source: Mayo Clinic (Williams Hematology7th ed. 2007) • M:F = 3:2 • 6th decade of life
ETIOLOGY • Somatic mutation on chromosome 9p which encodes tyrosine kinase-JAK 2 • Increased expression of protein tyrosine phosphatase activity of red cell precursors • Increased mRNA levels of PRV-1 gene granulocytes
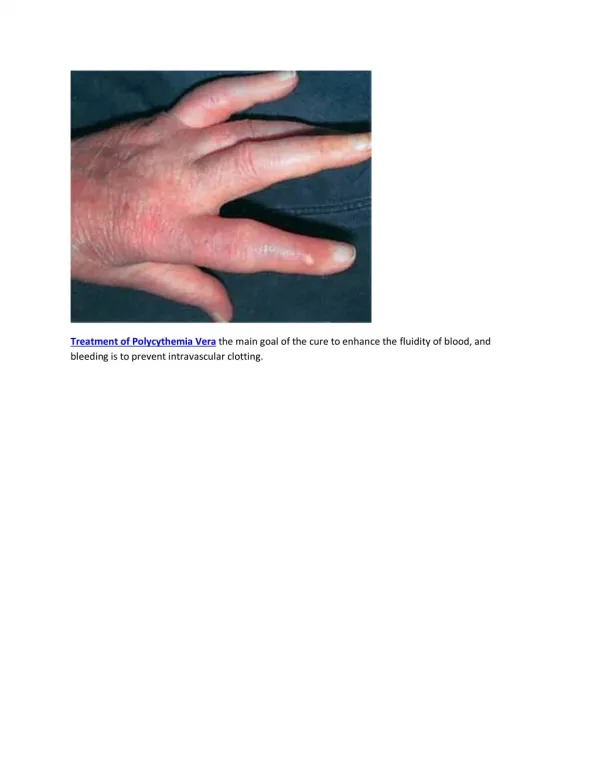
CLINICAL PRESENTATION • Insidious onset • Headache, plethora, pruritus, thrombosis, GI bleeding, gingival bleeding, weakness, dizziness and sweating
PHYSICAL EXAM • Splenomegaly – Present in 75% of patients at the time of diagnosis • Hepatomegaly – Present in approximately 30% of patients with polycythemiavera (PV) • Plethora , manifests in the face, palms, nailbeds, mucosa, and conjunctiva. • Hypertension
LABORATORIES • CBC = inc hct, inc hgb, inc wbc – absolute neutrophilia, inc platelets , inc RBC • PERIPHERAL BLOOD SMEAR = occasional myelocytes and metamyelocytes • Blood chemistry: Uric Acid: Hyperuricemia: • TIBC = high • Ferritin = low • EPO LEVELS = normal; <5IU/L • JAK2 = mutation • BONE MARROW ASPIRATION BIOPSY = hypercellular with involvement of all myeloid lineages
Patient • CBC = inc hct, inc hgb, increased wbc count but with absolute neutrophilia, inc RBC, normal platelets • PERIPHERAL BLOOD SMEAR = normocytic, normochromic, neutrophilic predominance • Blood chemistry: Uric Acid: Hyperuricemia • TIBC = not done • Ferritin = not done • EPO LEVELS = not done • JAK2 = positive for mutation • BONE MARROW ASPIRATION BIOPSY = not done
Patient’s Clinical Presentation • 64 years old • Male • Hypertensive (diagnosed 1990) • Plethoric • Gingival bleeding • Dizziness • (+) ecchymoses on both legs • (+) Grade 2-3/6 Holosystolic murmur • (+) Bipedal edema grade 1 • (-) Splenomegaly • (-) Hepatomegaly