Download
1 / 20
270 likes | 825 Vues
HAEMATURIA . HAEMATURIA. Common finding Incidental DEFINING HAEMATURIA Visible haematuria Non visible haematuria (dipstick and microscopic). Indication for urine dipstik testing. Lower urinary tract symptoms Upper urinary tract symptoms

E N D
HAEMATURIA • Common finding • Incidental • DEFINING HAEMATURIA • Visible haematuria • Non visible haematuria (dipstick and microscopic)
Indication for urine dipstik testing • Lower urinary tract symptoms • Upper urinary tract symptoms • Diagnosis of hypertension • Diabetes(at least annually) • Newly detected renal dysfunction(e GFR<60ml/min) • Suspected multisystem disease with possible renal involvement.
Innocent haematuria • Haemoglobinuria • Myoglobinuria • Menstruation • Sexual intercourse • Acute intermittent porphyria • Food :beet root, black berries, rhubarb • Drugs: nitrofurantoin,senna,rifampicin,phenolphthalein,chloroquine,doxorubicin • Chronic lead or mercury poisoning
HAEMATURIA • UTI typically causes non visible transient haematuria and if simple doesn't require further investigations. • Presence of bacterial peroxidases can cause a false positive dipstick test • Dipstick testing for blood is less sensitive in the urine with high specific gravity and heavy proteinuria
CAUSES OF HAEMATURIA • PRE RENAL CAUSES • Bleeding diathesis • Atrial fibrillation • Infective endocarditis • Scurvy • Purpura • Leukaemia • Thrombocytopenia • haemophilia
CAUSES OF HAEMATURIA • RENAL CAUSES • NEPHROLOGICAL • IgA nephropathy • Glomerulonephritis • Polyarteritis nodosa • Good pasture’s syndrome • Acute pyelonephritis • Polycystic kidney disease • Haemolytic uremic syndrome • Alport’s syndrome
Causes of haematuria UROLOGICAL GENERALIZED • Malignancy • Benign tumour • Trauma • Calculus • PKD • Renal vasculature problems • Medullary sponge kidney • Renal toxins • SLE
CAUSES OF HEMATURIA POST RENAL CAUSES URETERIC • Calculus • Carcinoma • Papilloma • schistosomiasis BLADDER/PROSTATIC • Tumour • BPH • Prostatic cancer • Calculus • Cystitis • Injury/FB • Purpura • Schistosomiasis
CAUSES OF HAEMATURIA URETHRAL • Acute urethritis • Calculus • Injury • Carcinoma • Papilloma • Urethral meatal ulcer • F.B
Approach to haematuria • Thorough history including • Urinary symptoms • Recent history (trauma/muscle injury/causes of factitious haematuria/exercise/foreign travel) • Systemic features (fever, weight loss) other symptoms(bleeding,bruising) • Co-morbidity • Drug history • Occupation • Family history
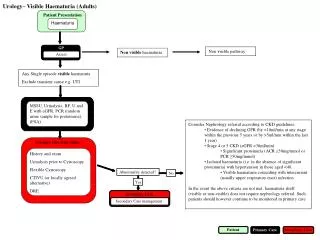
REFERRAL CRITERIA • URGENT (2 WEEKS WAIT) REFERRAL (urology) • Visible haematuria (unless GN is suspected) • Haematuria with recurrent or persistent UTI in adult over 40 years • Persistent non visible haematuria in adult over 50 years. • Abdominal mass identified clinically or on imaging that is thought to arise from urinary tract.
REFERRAL CRITERIA • UROLOGY • All patient with symptomatic non-visible haematuria who don't meet the criteria for urgent referral. • Patient with persistent asymptomatic non-visible haematuria age 40-50 years.
REFERRAL CRITERIA • NEPHROLOGY • Evidence of decline of eGFR (by >10ml/min in previous 5 years or by >5ml/min in the last year). • Stage 4 or 5 kidney disease. • Significant proteinuria (ACR 30 or more or PCR 50 or more). • Isolated haematuria with hypertension in those under 40 years. • Visible haematuria coinciding with intercurrent ,usually upper respiratory, infection.
If no cause established • Annual assessment(while haematuria persists)of BP, eGFR and ACR/PCR • Re referral to urology if; • Significant or increasing proteinuria(ACR>30 or PCR>50) • Estimated GFR <30ml/min(Confirmed on at least 2 readings and without an identifiable reversible cause) • Deteriorating eGFR(>5ml/min in 1 year or>10ml/min in 5 years.