Guillain-Barré syndrome (GBS)
160 likes | 1.61k Vues
Guillain-Barré syndrome (GBS). By Usman Bari #1054. IntroDuction. Fisrt described by Jean Landry in the mid 1800 ’ s and discovered in 1916 by Jean Alexandre Barre and Georges Gillain. (tests on soldiers) Rare – 1- 2 cases per 100,000 (most common non-trauma related paralysis)

Guillain-Barré syndrome (GBS)
E N D
Presentation Transcript
Guillain-Barré syndrome(GBS) By Usman Bari #1054
IntroDuction • Fisrt described by Jean Landry in the mid 1800’s and discovered in 1916 by Jean Alexandre Barre and Georges Gillain. (tests on soldiers) • Rare – 1- 2 cases per 100,000 (most common non-trauma related paralysis) • Guillain-Barré syndrome can affect anybody: age, sex, race. • inflammatory demyelinating polyneuropathy of the peripheral nerves
Signs and Symptoms • Ascending Paralysis - • Varying degrees of symmetric weakness with tingling sensations. These symptoms can increase in intensity until certain muscles cannot be used at all and, when severe, the person is almost totally paralyzed. • Dysfunction of the autonomic nervous system. Wide fluctuations in blood pressure, orthostatic hypotension, and sinus tachycardia among other cardiac arrhythmias. (65% of pts) • Loss of deep tendon reflexes, areflexia • Severe cases with loss of respiratory muscle weakness. . Such an individual is often put on a ventilator (30% of patients) to assist with breathing and is watched closely.
Pathophysiology • Not exactly known however is believed to have a multifactorial cause that is an auto-immune disease which occurs 3-4 weeks after an onset of gastrointestinal or respiratory viral infection (campylobacter jejuni, influenza virus, CMV). Sometimes also seen in after vaccination (1977 swine flu pandemic). • GBS onset is rapid, it can be from a few days to 4 weeks. • Through molecular mimicry the immune system attacks gangliosides.(GM1) Ganglioside-like epitopes exist in the bacterial wall of C. jejuni. • This leads to inflammation and demyelination of the peripheral nerves there isn’t any damage to the brain or spinal cord. (80% is myelin loss, 20% axon loss).
diagnosis Aside from the classic symptoms of GBS along with cranial nerve involvment bilateral weakness of facial muscles, CSF analysis and electrodianostic tests of nerves are needed. Tests: • CSF test through lumbar puncture shows increased protein levels with an absence of pleocytosis. (albiumino-cytological dissociation). Normal protein levels ( 15-60 mg/dL) in the first week but they significantly increase by 90% by the end of second week (100-1000mg/dL). • Nerve conduction tests: prolonged distal latencies, conduction slowing, conduction block • Electromyography
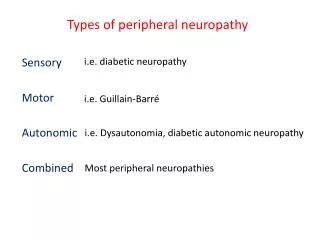
Differential diagnosis • Poliomyelitis • Botulism • Myasthenia Gravis • Porphyria polyneuropathy
Variations of GBS • Acute inflammatory demyelinating polyneuropathy (AIDP) – against schwann cell membranes • Acute motor axonal neuropathy (AMAN) – against nodes of ranvier • Acute motor sensory axonal neuropathy (AMSAN) – similar to AMAN but with severe axonal damage • Miller Fisher syndrome (MFS)
Management/ treatment • Regular monitoring to prevent potentially fatal complications: • Monitoring respiratory function (vital capacity, respiation frequency) may be need to put on ventilatory support. • Regular check for autonomic dysfuntion (ECG, pulse and blood pressure) • Physical therapy (mobilization for DVT) • Plasmaphpheresis • Intravenous Immunoglobulin (IVIg) – high dose every 3 to 4 weeks
Prognosis/ complications • Prognosis is usually good if managed well. 80% fully recover after the onset of the 4th week of GBS. The recovery period can take anywhere from a few months to a year. • Minor fiindings such as areflexia may persist. 5 - 10% develop one or more recurrent episodes, which is classified as chronic inflammatory demyelinating polyneuropathy.
Case Study • A 23-year-old man with a recent history of a viral-type illness presents to the emergency department because of complaints of weakness in his legs. He is admitted to the hospital and the weakness progresses into his thighs and hips. What is his prognosis? • A. Fair, with treatment the progression of the muscle weakness will stop, but the weakness will remain for the remainder of his life • B. Good, with treatment the muscle weakness will definitely stop and not progress further • C. Good, with treatment the condition will run its course, and his life can be saved and he should have no residual sequelae • D. Dismal, the condition will continue to progress, involving his respiratory muscles, causing his death even if treated
references • http://www.med.unc.edu/pedclerk/schedules/clerkship-at-moses-cone/readings-and-resources/clinical-problem-solving-conferences-readings/14.%20Guillain-Barre%20syndrome.pdf • http://www.youtube.com/watch?v=c-8ia81XPMw • http://www.webmd.com/brain/tc/guillain-barre-syndrome-topic-overview • http://www.uptodate.com/contents/pathogenesis-of-guillain-barre-syndrome-in-adults