Download
1 / 30
300 likes | 676 Vues
AN UNUSUAL DIAGNOSIS MADE ON PAP SMEAR. HISTOPATHOLOGY DEPARTMENT HOLY FAMILY HOSPITAL DR. HAJRA AZHAR. The pap test ; Effective way to screen women for squamous dysplasia and carcinoma of uterine cervix. Primarily used to detect epithelial abnormalities,

E N D
AN UNUSUAL DIAGNOSIS MADE ON PAP SMEAR HISTOPATHOLOGY DEPARTMENT HOLY FAMILY HOSPITAL DR. HAJRA AZHAR
The pap test ; • Effective way to screen women for squamous dysplasia and carcinoma of uterine cervix. • Primarily used to detect epithelial abnormalities, • Certain infections can easily be detected by Pap smear.
Pap smear…. • In the year 2015 ; • A total of 469 cases of cytology were received in the department of Histopathology, Holy Family Hospital • Out of these , 287cases were Pap smears. • we are presenting today, a rare and interesting case of an infectious disease that we picked on Pap smear.
HISTORY A 40 years old female presented in gynaeOPD with the complaints of : • Foul smelling vaginal discharge • Abdominal distension • Abdominal pain Four months • Vomiting • Loss of appetite
HISTORY….. No history of : • Bleeding per vagina • Itching • Weight loss • Fever • Night sweats • Tuberculosis in the family or • Past history of tuberculosis.
MENSTRUAL HISTORY • She has secondary amenorrhea for the last 10 years. • GYNAECOLOGICAL HISTORY • Post coital bleeding, superficial dyspareunia • PAST MEDICAL AND SURGICAL HISTORY • FAMILY HISTORY NOT SIGNIFICANT • PERSONAL HISTORY
EXAMINATION • GENERAL PHYSICAL EXAMINATION A middle aged lady with normal vital signs. • BP = 110/70 • PULSE = 84/min • TEMP = 98.6 º F • R/R = 24/min • Pallor + • Jaundice º • Cyanosis º • Clubbing º • Oedema º • Lymph nodes º
PER SPECULUM EXAMINATION; PER SPECULUM EXAMINATION; • An unhealthy looking cervix , grossly erythematous, congested and bled on touch. • There was white colored , foul smelling discharge. • On Vaginal examination; • A normal sized retroverted uterus, which was freely mobile. • No adnexal mass or forniceal tenderness.
Rest of the systemic examination; • unremarkable.
INVESTIGATION PLAN Considering the state of cervix, investigations planned by gyne dept. were : • All baseline investigations • Pap Smear • HVS C/S • Abdomino - pelvic ultrasound • CT Scan • Examination under anesthesia & cervical biopsy
BASELINE INVESTIGATIONS…. • Blood CP ; • TLC 10,000 /ul • RBC 413,000 /ul • Hb 9.4 g/dl • Plts 778/ul • MCV 66 fl • MCH 22.7 pg • MCHC 34.5 g/dl
BASELINE INVESTIGATIONS…. Cont… • LFTs • ALT 12 IU/l • ALP 89 IU/l • TOTAL BILIRUBIN 4 umol/l • RFTs • SERUM UREA 15mg/dl • SERUM CREAT 0.7mg/dl • URIC ACID 2.3mg/dl
BASELINE INVESTIGATIONS…. • PT/APTT • PT 15/14 • APTT 40/32 VIRAL SEROLOGY • Anti HbsAg Negative • Anti HCV Negative
HVS C/S • No growth wasobtained after 24 hours at 37ºC Aerobic Incubation.
ABDOMINOPELVIC ULTRASOUND • Cervix • Cervix appeared irregular. An echomixed area measuring 3.3 x 2.6cm was seen. • CUL- DE-SAC • Free fluid was seen. • IMPRESSION • Normal Abdominal ultrasound • Cervical growth
CT SCAN • Heterogeneously enhancing circumferential thickening of cervical canal is seen resulting in near total occlusion of cervical canal suggesting cervical growth. • A well-defined, dense calcified lesion in the pelvis, in cul-de-sac closely abutting uterine wall is also seen ( Could be a calcified lymph node / calcified fibroid).
EXAMINATION UNDER ANESTHESIA • UTERUS - • 14 weeks size, freely mobile • A nodular growth occupying whole of the endocervical canal is present. Cervical lips appear normal. • Clinically the lesion is most likely ADENOCARCINOMA OF CERVIX. • ADENEXA - • Clear • Pap smear - was taken & sent to lab • Biopsy - was taken from several points of growth and sent for histopathology.
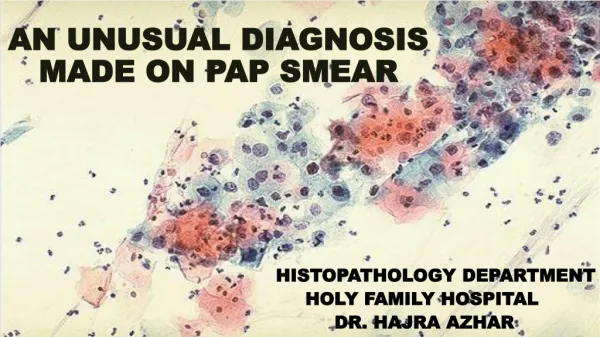
PAP SMEAR MORPHOLOGICAL FEATURES; Smear is adequate for interpretation and shows marked inflammation. Multiple epitheloid granulomas and multinucleated giant cells are also present. No dysplastic cells seen. • CYTOLOGICAL DIAGNOSIS: - CONSISTENT WITH TUBERCULOUS CERVICITIS
FINAL DIAGNOSIS; CERVICAL TUBERCULOSIS
GENITAL TUBERCULOSIS • Genital tuberculosis (TB) in females is not uncommon, particularly in communities where pulmonary or other forms of extragenital TB are common. • TB can affect any organ in the body, can exist without any clinical manifestation, and can recur. • Female genital TB is typically understood as a disease of young women, with 80% to 90% of cases diagnosed in patients 20–40 years old, often during workup for infertility.
INCIDENCE ; • Varies with geographic location & range from 10.3% inIndia to less than 1%in America & Sweden • Increasing in developed countries due to its association with HIV. • World wide incidence of genital tuberculosis in infertile womenis 5 – 10 %, A study in Pakistan shows 20%. • The frequency of involvement of various genital organs : • Fallopian tube 90-100% • Endometrium 50-60% • Ovaries 20-30% • Cervix 5-15% • Vulva and vagina 1%
PATHOGENESIS ; Pelvic tuberculosis ; • Is produced by - Mycobacterium tuberculosis or Mycobacterium bovis. • Pelvic organs - are infected from a primary focus, (usually chest), by hematogenousspread. • The cervix can be infected by; • lymphatic spread or bydirect extension. • In rare cases, cervical TB may be a primary infection, introduced by a partner with tuberculous epididymitis
SIGNS AND SYMPTOMS • Abnormal vaginal bleeding • Menstrual irregularities • Abdominal pain • Constitutional symptoms The macroscopic findings ;- • Papillary or vegetative growths & ulceration • May be misinterpreted as invasive carcinoma of cervix.
DIAGNOSIS • Diagnosis of cervical TB : • Histopathology - caseating granulomas are diagnostic. • Staining for acid fast bacilli – may not be very useful • Isolation of mycobacterium on culture - gold standard • one third of cases - are culture negative, So, presence of typical granulomata is considered sufficient for diagnosis. • Newer modalities like ELISA - can aid in the diagnosis.
Take home message; • Tuberculous cervicitis ; - can be clinically , misdiagnosed as cervical carcinoma. • Pap smear – • Is mostly used for the detection of early cervical carcinoma , • it can also diagnose tuberculosis of cervix and certain other infections. • Recognition of these rare conditions : • will decrease the potential for misdiagnosis and • expedite appropriate management of pts with these conditions.
REFERENCES • Chowdhury NN. Overview of tuberculosis of the female genital tract. J Indian Med Assoc. 1996;94:345–6. 361. [PubMed] • 2. Carter JR. Unusual presentations of genital tract tuberculosis. Int J Gynaecol Obstet. 1990;33:171–6.[PubMed] • 3. Bhalla A, Mannan R, Bhasin TS. Tubercular cervicitis clinically mimicking as carcinoma cervix: Two case reports. J ClinDiagn Res. 2010;4:2083–86. • 4. Sinha A, Banerjee N, Roy KK, Takkar D. Cervical tuberculosis mimicking carcinoma cervix. J ObstetGynecol India. 2002;52:154. • 5. Singhal SR, Chaudhry P, Nanda S. Genital tuberculosis with predominant involvement of cervix: A case report. Clin Rev Opin. 2011;3:55–6. • 6. Nabi U, Umber F, Nafees M, Khurshid N. Tuberculosis of cervix: A rare clinical entity. Int J Pathol.2012;10:41–3. • 7. Lamba H, Byrne M, Goldin R, Jenkins C. Tuberculosis of the cervix: Case presentation and a review of the literature. Sex Transm Infect. 2002;78:62–3. [PMC free article] [PubMed]