Rift Valley Fever
370 likes | 1.41k Vues
Rift Valley Fever. Sherine Shawky, MD, Dr.PH Assistant Professor Department of Community Medicine & Primary Health Care College of Medicine King Abdulaziz University shshawky@hotmail.com. Rift Valley Fever. Acute febrile viral disease Affecting animals & humans

Rift Valley Fever
E N D
Presentation Transcript
Rift Valley Fever Sherine Shawky, MD, Dr.PH Assistant Professor Department of Community Medicine & Primary Health Care College of Medicine King Abdulaziz University shshawky@hotmail.com
Rift Valley Fever • Acute febrile viral disease • Affecting animals & humans • Causes influenza-like illness • May lead to high morbidity, mortality & economic loss
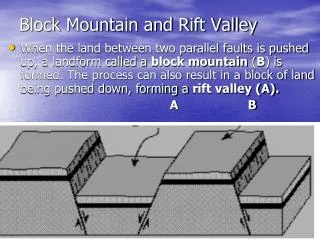
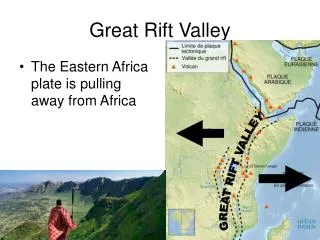
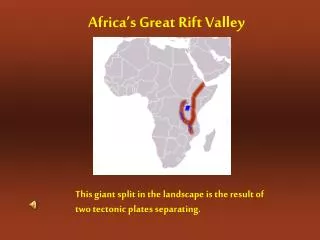
Geographic Location & Geologic Feature of Rift Valley • Length: 6,000miles • Site: Lebanon to Mozambique • Largest part: Kenya • Development: Subterranean forces • Feature: Dambos
Causes of Outbreaks Rainfall or Inundation Wetlands & Stagnant water Vegetation Growth Flourishing of mosquitoes Transmission of Infection
RVF Virus Glyco- protein spikes Lipid envelope L S G1 M G2 transcriptase Coiled nucleocapsid RNA+N protein
Mode of Transmission • Mosquitoes • Other blood suckling insects • Contact with blood or other body fluids of infected animals • Consumption of infected milk
Mode of Transmission(cont.) • Contact with blood or other body fluids of infected humans in late stages of disease • Airborne transmission • Inoculation through broken skin
Target • Liver: focal necrosis • RBCs: haemagglutination • Brain: necrotic encephalitis
Clinical Picture 1- Non-Human Host • Fever • Hepatitis • Abortion • Death • Adults: 10-30% • Neonates: 100%
2- Human Host • Incubation period of 2-6 days • Asymptomatic • Flu-like illness • Abdominal pain • Photophobia • Recovery in 2-7days
Rate: 0.5-2.0% Onset: 1-3 weeks Presentation Localized pain Blurred vision Loss of vision: 1.0-10.0% Lesions: Macular lesions Retinitis Retinal detachment Death: rare Complications of RVF 1- Ocular Lesions
Rate: < 1.0% Onset: 1-3 weeks Death: rare Presentation: Severe headache Vertigo Seizures Coma 2- Meningoencephalitis
Rate: < 1.0% Onset: 2-4 days Presentation: hemorrhagic phenomenon Lesions: Acute fulminant hepatitis DIC Hemolytic anemia CFR: 50.0% 3- Haemorrhagic fever
High Risk Groups • People who sleep outdoors at night • Slaughterhouse workers, butchers veterinarians and others who handle blood, other body fluids or tissues of infected animals
High Risk Groups (cont.) • Doctors and nurses in contact with infected cases at late stages of the disease • Laboratory technicians • Travellers visiting epidemic areas
Diagnosis of RVF • Antibody detection • ELISA • EIA • Virus detection • Virus isolation • Antigen detection • PCR
Prevention & ControlI. Animal • Vaccination of unaffected animals • Live attenuated vaccine • Killed vaccine • Notification of affected animals • Application of safe insecticides to eradicate blood suckling insects
I- Animal(cont.) • Periodic surveillance of susceptible animals to assess immune status • Application of quarantine measures for testing of imported animals • Rapid burial of dead bodies
II- Vector • Removal of stagnant water • Weekly treatment of water collections using insecticides • Application of insecticides every other day in all gardens • Removal of objects that can act as possible water containers
III- Humans: 1- General Measures • Sleeping indoors • Using bed nets during sleep • Putting screens on windows • Wearing clothes that protects whole body
III- Humans: 1-General Measures (cont.) • Applying mosquito repellents • Using spray on clothes • Avoiding peaks of mosquito activity • Avoiding presence near vegetations in the evening
III- Humans1-General Measures (cont.) • Avoiding direct contact with animals • Washing hands after contact with animals, their blood or other body fluids • Avoid drinking raw milk
III- Humans2- Community Measures • Health education • Epidemiologic research program • Active disease surveillance • Check measures at air, sea and land entry points
III- Humans3- Occupational Measures • Wearing masks, gloves, gowns and other barriers according to infected host’s condition • Laboratory samples should be handled by trained staff
III- Humans3- Occupational Measures (cont.) • Application of water, soap and antiseptic solution on exposed parts • Application of copious water and eye wash solution on exposed conjunctiva
Management of Suspected Cases • Notification • Ascertainment of cases • Identification, screening and surveillance of contacts
CBC Urea Creatinine AST, ALT ALP,Bilirubin Albumin PT & PTT LDH & CPK Hepatitis A IgM & IgG, HBsAg, HBcAB, HCV Ab RFV seriology & viral culture Recommended Investigations For Suspected Cases
Management of unhospitalised Patients • Isolation at home • Contacts should wear masks, gloves and protective clothes • Safe disposal of patients linens & clothes • Close follow-up for 6 weeks
Shock Decreased urine output AST & ALT > 200U/mL Bilirubin>100 mol/L Thrombocytopenia< 100,000/mm3 Anaemia< 8gm/dL Creatinine>150mol/L Confusion or other CNS manifestation Evidence of DIC Indications For Hospitalisation
Management of Hospitalised Patients • General Supportive Measures • Isolation in negative airway pressure room • Safe disposal of soiled linens • Safe disposal of solid medical waste • Safe sewage disposal
Management of Hospitalised Patients (cont.) • Ribavirin, Interferon, Immune Modulators & Convalescent Phase Plasma give promising results • Introduction to ICU or haemodialysis unit if indicated
Hospital discharge after: • Improvement in general status • Decline in liver symptoms • Recovery from DIC • Follow-up in ophthalmology and medical clinics for 6 weeks • Safe burial practice for dead cases
Conclusion • RVF is spreading outside Africa • Although often mild, may lead to high morbidity and mortality • No vaccine for humans • No specific treatment • Preventive measures are crucial