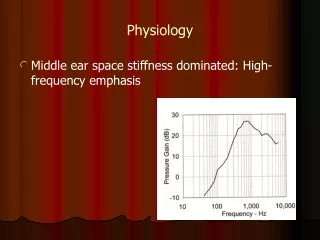
Physiology 441
Physiology 441. The Renal System, Chp. 14 Text: Human Physiology (Sherwood), 6 th Ed. Julie Balch Samora, MPA, MPH jbsamora@hsc.wvu.edu 293-3412, Room 3145. Medullary vertical osmotic gradient.

Physiology 441
E N D
Presentation Transcript
Physiology 441 The Renal System, Chp. 14 Text: Human Physiology (Sherwood), 6th Ed. Julie Balch Samora, MPA, MPH jbsamora@hsc.wvu.edu 293-3412, Room 3145
Medullary vertical osmotic gradient • The medullary vertical osmotic gradient and ADH allow the kidney to excrete urine of varying concentrations • Without this osmotic gradient, we could not produce a concentrated urine, and would be unable to conserve water • We would likewise be unable to rid the body of excess water w/o this system
Distal tubule Distal tubule Glomerulus Proximal tubule Bowman’s capsule Proximal tubule Cortex Medulla Loop of Henle Collecting duct Descending limb of loop of Henle Other nephrons emptying into the same collecting duct Vasa recta Ascending limb of loop of Henle To renal pelvis Fig. 14-5, p. 505
Countercurrent Multiplication • The loops of Henle of the juxtamedullary nephrons are responsible for establishing the concentration gradient in the renal medulla • Descending limb is freely permeable to H2O, but NOT NaCl – so H2O goes into IF • Ascending Limb IMPERMEABLE to water • The ascending limb actively transports out NaCl
Renal Disease • Acute – sudden shutdown of kidneys; may be reversible • Chronic – progressive, slow, insidious, irreversible loss of kidney fxn. Up to 75% of kidney tissue can be destroyed before loss of kidney fxn is even noticeable • End stage renal failure – when 90% of kidney fxn has been lost
Consequences of Renal Failure • Uremic toxicity – retention of waste products – body overwhelmed by toxins • Metabolic acidosis – results from the inability of the kidneys to adequately secrete H+ - leads to CNS depression • Potassium retention – from inadequate tubular K+ secretion – altered cardiac excitability
Consequences of Renal Failure • Sodium imbalances – from inability of kidneys to vary Na+ reabsorption • Phosphate and calcium imbalances – from impaired reabsorption – leads to skeletal disturbances • Loss of plasma proteins – from leakiness of glomerular membrane – leads to edema • Inability to vary urine concentrations – from impairment of countercurrent system
Consequences of Renal Failure • Hypertension – from salt and fluid retention and excess angiotensin II • Anemia – deficiency of erythropoietin • Depression of immune system – toxic effect on immune system – ↑ infxns
Micturition • Transmission of urine to the bladder • Urine forced along ureters by peristalsis • Ureters penetrate bladder obliquely, preventing reflux • As bladder fills, the ureteral openings are compressed • Even though urine can still enter bladder through compressed openings, urine cannot escape back up ureters
Micturition • Storage of urine • The bladder wall, made of smooth muscle, can stretch without a concomitant build-up of intrabladder pressure • Once bladder fills beyond 200-400 ml, the pressure rises, stretching receptors • Internal urethral sphincter – at end of bladder, closes off • Bladder supplied by PNS
Micturition • Role of the external urethral sphincter • Farther down the urethra is a circular layer of skeletal muscle • This sphincter is supplied by a motor neuron • Unless the motor neuron is inhibited, it fires continuously, keeping the external sphincter contracted, thereby preventing urine from leaving bladder
Micturition Reflex • When stretch receptors within the bladder wall are stimulated, the micturition reflex is initiated • Afferent fibers from the stretch receptors stimulate the PNS to inhibit the motor neuron supplying the external urethral sphincter • In response to PNS stimulation of the bladder, it contracts.
Micturition Reflex • As the bladder contracts, the internal urethral sphincter is pulled open mechanically • Inhibition of the motor neuron supplying the external sphincter allows for relaxation • Both sphincters are relaxed, bladder is contracting, and urine flows freely from the bladder through the urethra • Entirely a spinal reflex!
Voluntary Control of Micturition • Must be learned • Can override the micturition reflex • One can delay micturition despite synaptic input from bladder stretch receptors • Although internal sphincter is open, can keep the external sphincter contracted so no urine is expelled
Review Questions • What gives rise to the unique appearance of the kidney? • What is the average GFR?
Review Questions • What is the role of the vasa recta? • What is the importance of the vertical osmotic gradient?
Review Questions • What is the major force favoring glomerular filtration? • A decrease in afferent arteriolar resistance will do what to the GFR?
Review Questions (T/F) • The kidney eliminates toxins such as urea, uric acid, glucose and creatinine • The kidney plays a role in the body’s vitamin D concentration • The kidney produces renin
Review Questions • What are the types of autoregulation in the kidney? • Where is sodium reabsorbed?
Review Questions (T/F) • Most of the filtered plasma is excreted • Glomerular filtration is a highly discriminating process • The higher the BUN, the better function the kidneys have
Review Questions • What is an example of a substance that is both actively secreted and actively reabsorbed? • What is the formula for FF?
Review Questions • If a gentleman’s avg. GFR is 125 ml/min, a substance that is being reabsorbed would have a clearance rate that is ↑, ↓, or ↔ compared with his avg. GFR. • What establishes the medullary vertical osmotic gradient via the countercurrent multiplication?
Review Questions (T/F) • The ascending limb of the loop of Henle of a juxtamedullary nephron is permeable to water. • The glomerular capillary pressure is lower than capillary pressure elsewhere in the body
Review Questions (T/F) • Water moves by osmosis from an area of lower osmolarity to an area of higher osmolarity • ADH is secreted during water excess
Review Questions (T/F) • The amount of glucose filtered is directly proportional to the plasma glucose concentration • Upon entering the distal tubule, the tubular fluid is hypertonic
Review Questions (T/F) • Potassium is filtered and both actively reabsorbed and actively secreted • Urea is filtered and actively reabsorbed • What substance is filtered, and completely reabsorbed (under nrml conditions)?