Download
1 / 50
500 likes | 692 Vues
Development and evaluation of an E-health system to care for patients with bladder pain syndrome/interstitial cystitis (BPS/IC). Yung-Fu Chen ( 陳永福 ), Ph.D. Professor, Department of Healthcare Administration, Central Taiwan University of Science and Technology, Taichung;

E N D
Development and evaluation of an E-health system to care for patients with bladder pain syndrome/interstitial cystitis (BPS/IC) Yung-Fu Chen (陳永福), Ph.D. Professor, Department of Healthcare Administration, Central Taiwan University of Science and Technology, Taichung; Adjunct Professor, Health Services Administration, China Medical University, Taichung
Outline • Introduction • Methods • Preparation of health educational materials • Management of symptom flares • Participants and protocol • Experimental design • Statistical analysis • Results • Discussions • Conclusion • Future Works
Behavior Change • Acquisition of diseases and causes of their mortality and morbidity are related to behavior (Parkin, Boyd & Walker 2011) • Appropriate interventions administrated to change behavior are essential in preventing occurrences or recurrences of diseases • Clearly identifying the active components when designing, evaluating, and reporting interventions is important for understanding principles of behavior change (Michie & Johnson 2012) 4
Behavior Change Intervention • Regarding the 7 behavior topics, i.e., unintentional injury, peer violence, dating/intimate partner violence (IPV), mental health, smoking, alcohol/substance use, and safe sex, patients are interested in receiving technology-based behavior interventions, including computer, Internet, social networking, mobile phone, and text messaging, on each topic (Renney et al. 2012). • 89.6% reported preference for at least one behavior topic • >50% reported preference for each specific topic • The effectiveness of Internet-based interventions was enhanced by additional communicating techniques, especially the short message service (SMS) or text messaging (Webb et al. 2010)
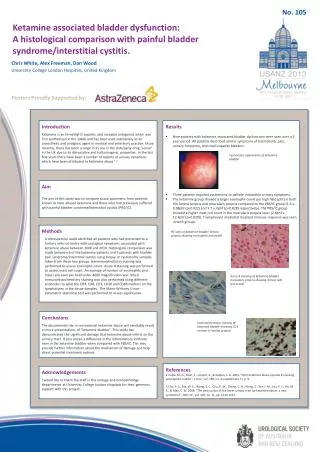
Bladder Pain Syndrome/Interstial Cystitis (BPS/IC) • BPS/IC is a poorly defined chronic bladder disease characterized by pelvic pain and urinary storage symptoms (e.g. urgency and frequency) in the absence of proven urinary infection or other definable pathological etiology (Hanno et al. 2011). • The etiologies of the disease are multifocal, whether it has originated from the bladder or other pelvic organs, or is a systematic disease is still not elucidated (Moutzouris & Falagas 2009) 黏膜受損 膀胱擴張術黏膜出血情形 6
BPS/IC • Currently, no single therapy has been found to be effective for the majority of patients (Hanno et al. 2011) • Clinically, the patients have been bothered by the disease for a long time, making them feel frustrated when receiving further therapies. • Recently, environmental factors, such as dietary, physical activity, smoking and drinking behaviors, attributed substantially to the occurrence of BPS/IC based on the twin studies (Altman et al.2011; Tunitsky et al.2012) 7
SMS Intervention • When the symptoms flare up, most patients cannot follow the regiments of self-management and usually seek help by visiting the emergency department without receiving effective treatment, resulting in a waste of medical resources and degradation of quality of life. • Intervention by sending simple messages through cellular telephones and the Internet can effectively decrease blood pressure, reduce bodyweight and waist circumference, decrease blood glucose levels of obese type 2 diabetes patients, and promote safer sex and sun safety (Kim & Kim 2008; Gold et al. 2011). 8
Motivations & Objectives • It is currently impossible to completely cure BPS/IC disease because of unclear pathogenesis; the treatment is mainly to alleviate symptoms or to improve QOL • Treatment of BPS/IC needs a lot of healthcare resources and might cause a great burden for the country as a result of its chronicity; • Intervention using mobile telephone and the Internet is effective in caring for patients with chronic diseases in outpatient settings. • The objective is to develop an E-health system by integrating mobile telephone and the Internet to through weekly health education by asking patients to check their daily foods, activities and living habits. 9
Materials and MethodsPreparation of health educational materials (1) Appendix I: Weekly check for consolidating good habits promoted by health education 11
Materials and MethodsPreparation of health educational materials (2) 12
Preparation of health educational materials (1) • Items 1, 3, & 4: The BPS/IC patients are generally sensitive to foods containing vitamin C, potassium, or spices, as well as beverages containing caffeine or alcohol (Friedlander et al. 2012) • Item 2: To reduce the recurrence of BPS/IC symptoms, the patients are encouraged to drink 1500 cm3 water daily (ICA: http://www.ichelp.org/). • Item 5: Smoking is associated with a higher risk of BPS/IC (Tettamanti et al. 2011) • Items 6 & 7: Certain types of exercise, such as pelvic floor muscle exercise, and wearing of tight-fitting clothes might worsen BPS/IC symptoms in some patients (Hanno PM, et al. 2011). Yoga can be carried out as a complementary and alternative therapy for patients with anxiety (Sharma & Haider 2013) 13
Preparation of health educational materials (2) • Items 8 & 13: The patients are encouraged to bath their whole lower abdomen with warm water (40°C) more than once a day, each time lasting for 15 min. A heat pad can also be placed over the abdomen to relieve uncomfortable symptoms (ICA). • Item 9: More than 80% of premenopausal IC women have symptoms flare up before, within, and after the menstrual cycle, and 35% of IC women choose heating bag to relieve pain (Peters et al. 2008). • Items 10–12: Treatment and care of the vagina and genital area might affect sexual and reproductive morbidities for women (Hilber et al. 2010) • Item 13: Guided imagery or meditation was shown to be effective in pain and symptom management for BPS/IC patients (Carrico et al. 2008) 14
♥ ♥ ♥ Mobile Phone Pre- & Post-test Management of Emergent Symptom Flares Web Service Survey by Questionnaires Weekly Health Education Materials and Methods ICT Intervention (1) 15
Materials and MethodsICT Intervention (2) Independent Variable Dependent Variable 16
Materials and MethodsManagement of symptom flares • An SMS application was designed to provide a Q/A service to handle the cases of symptom flares. • When an emergent symptom occurred, the patient was encouraged to send a message by typing the event number (Appendix II) to the SMS server through a designated mobile phone number. • The template contains the questions (symptoms) and their corresponding answers. • The SMS server responded to the question by sending its corresponding answer to guide the patient on how to relieve the symptom. 17
Internet Materials and MethodsManagement of Symptom Flares Question Base Station Mobile phone Message Center (China Telecom) Internet Web Application WebServer 手機 先喝大量水 xxxxxx Internet Base Station Message Center (China Telecom) Internet Response 18
Control Group Materials and MethodsParticipants and protocol A total of 80 BPS/IC patients were recruited and randomly assigned to either study or control group. The study was approved by the IRB of Taichung Hospital. Study Group 40 Patients 7 were excluded 40 Patients 8 were excluded Traditional treatment Weekly health education Urgency Management Traditional treatment None None
BaselineW8 Control Group F1~F3 E E R+F1~F3 BPS/IC Patients R R R R Study Group BaselineW8 W1 W2 W3 W4 F: Questionnaires F1:SF-36 F2:O’Leary-SantSymptom Index and Problem Index Scale F3:VAS scale of Pain & Urgency Baseline: F1-F3 & CytoscopicHydrodistension (Anesthetic Bladder Volume) R: Weekly Health Education E:Emergency Intervention Materials and MethodsExperimental Paradigm (1) . . . . .
Materials and Methods Experimental Paradigm (2) • Heath management: 台灣間質性膀胱炎關懷協會(Taiwan Interstitial Cystitis Association)website (http://taic.hopto.org). Health Education & Management 22 22
SF-36Survey Materials and Methods Experimental Paradigm (3) 23
O’Leary-Sant Index VAS Pain & Urgency Scale Materials and Methods Experimental Paradigm (4) 24
Materials and MethodsStatistic Analysis • Descriptive statistics were used to analyze the demographic information, disease severity and questionnaires of the recruited patients • Inferential statistics (Student’s t-test) were applied to compare the improvement of health status and symptoms between the study and control groups, as well as between pre-test and post-test for both control and study groups. • SAS (SAS Institute Inc., Cary, NC, USA) was used as the tool for statistic analysis. 25
ResultsComparison between study and control groups Table 1. Comparison of demographic information, bladder volume, and disease severity 27
ResultsComparison between study and control groups Table 1 (Cont.). Comparison of SF-36 survey 28
ResultsComparison between study and control groups Table 2. Comparison of SF-36 survey before and after ICT intervention 29
ResultsComparison between study and control groups Table 3. Comparison of disease severity before and after ICT intervention 30
DiscussionPrevalence • The prevalence in Asian countries investigated based on O’Leary-Sant indices is lower than the European countries (0.31-0.68%) and the USA (0.57%) • 0.26% in South Korea (Choe et al. 2011), 0.27% in Japan (Inoue et al. 2009), and 0.27% in Taiwan (Lee 2009) • Different diagnostic criteria might be the reason causing such a difference even investigated by the same research groups (Rosenberg and Hazzard 2005, Rosenberg et al. 2007); • Rosenberg and Hazzard (2005) presented a prevalence of 0.57% investigated based on O’Leary-Sant indices and Pelvic pain and Urgency/Frequency (PUF) score only, while it significantly increased to 4.3% with the diagnosis based on the patient history, PUF score, patient interview, and test results of potassium sensitivity test or anesthetic bladder challenge (Rosenberg et al. 2007). 32
DiscussionDyspareunia • Dyspareunia is widely observed in female BPS/IC patients, with pain as the most important finding significantly degrading the quality of life (Srivastava et al. 2011). • It was estimated to occur in 49–90% of the BPS/IC patients; among them, 54% intended to avoid intercourse most of the time because of the pain incurred (Wehbe et al. 2010). • Female BPS/IC patients experienced a much higher level of sexual dysfunction, such as lack of interest in sex, arousal difficulties and pain, compared with the general population (Kellogg-Spadt & Whitmore 2006). • Pain during intercourse is a strong indicator of poor QOL for BPS/IC patients (Bogart et al. 2011). Hence, reminding the patients to use lubricant and change position during intercourse, and to clean the vulva and bath the abdomen with warm water after intercourse, is believed to be effective in reducing pain during and afterintercourse. 33
DiscussionHealth Education (1) • Around 90% of the IC/BPS patients complain sensitive to diet foods, e.g. citrus fruits, tomatoes, foods containing vitamin C, drinks, e.g. coffee, tea, carbonated and alcoholic beverages, and spicy foods (Friedlander et al. 2012, Bassaly and Downes 2011). Gleason et al. (2012) reported that high caffeine intake is associated with an increase in the incidence of urgency inconsistence, which is consistent to the finding of Jura et al. • Smoking is associated with a higher risk of BPS (Tettamanti et al. 2011), LUTS (Maserejian et al. 2012), and overactive bladder (Dallosso et al. 2003) in women. 34
DiscussionHealth Education (2) • Certain type of exercise, such as pelvic floor muscle exercise, and wearing of tight-fitting clothes may worsen IC/BPS symptoms in some patients (Hanno et al. 2011). • A low level of physical activity was reported to be associated with 2-3 times higher likelihood of LUTS symptoms, while high level of physical activity was found to be inversely associated with total LUTS, as well as voiding but storage symptoms in women (Maserejian et al. 2012). • Hence, regular mild aerobic exercises, such as yoga, hiking, jogging, etc., reaching a high level of PASE (physical activity scale for the elderly) score (Washburn et al. 1999) are believed to be able to reduce IC/BPS re-occurrence. • Guided imagery or meditation was demonstrated to be effective in pain and symptom management for IC/PBS patients (Carrico et al. 2008). 35
DiscussionHealth Education (3) • Patients who understand the information and own the knowledge related to a disease can facilitate behavior change and disease management. SMS was shown to be effective in improving healthcare processes and outcomes (Krishna et al. 2009, Liang et al. 2011) • A good habit or behavior, such as eating, drinking, or exercising behavior, will be formed in a period ranging from 18 to 254 days with a median of 66 days for participants with good fits (Lailly et al. 2010). 36
DiscussionICT Intervention • It was reported that administration of daily educational text messages with SMS improved knowledge and facilitated continuous use of oral contraceptives (Castaño et al. 2012, Hall et al. 2012) • In contrast, face-to-face behavior counseling accompanied with phone interviews didn’t show improved adherence of oral contraceptives among young women (Berenson & Rahman 2012). • Text messaging reported to be able to deliver sensitive information, such as sexual health, in an cost-effective and efficient way might be the reason causing such a discrepancy (Lim et al. 2008). 37
Conclusion • In conclusion, the E-health system supporting health education and providing SMS for self-management was demonstrated to be effective in improving QOL and alleviating symptoms for the patients with BPS/IC. • The Internet healthcare education is useful to consolidate patients’ healthy dietary habits and life styles, as well as to self-manage their outbreak symptoms. 38
Future Works • The intervention based on video-tailored physical activity was reported to be feasible in terms of user preference (Vandelanotte and Mummery 2011). • Almost all the participants in the focus group agreed with the video-tailor intervention, and around 36% of the survey participant favored a video-based over a text-based intervention. • When designing a video, most survey participants preferred a role model to present the personal physical activity. • Intervention based on videos with the physicians as the main role is expected to be more effective in the treatment of chronic diseases. • To build all the functions in a smartphone App is expected to be more effective in health education and disease management. 39
References • Alfven G (2010) SMS pain diary: a method for real-time data capture of recurrent pain in childhood. ActaPaediactrica 99, 1047-1053. • Bal, E. (2007). An RFID application for the disabled: path finder. In Proceedings of IEEE International Conference on RFID Eurasia, 1-5. • Butrick CW. (2003). Interstitial cystitis and chronic pelvic pain: New insights in neuropathology, diagnosis, and treatment. ClinObstetGynecol, 46, 811-23. • Canavan TP., Heckman CD. (2000). Dyspareunia in women. Breaking the silence is the first step toward treatment. Postgrad Med, 108, 149-52.157-60, 164-6. • Clemens J. Q., Stoto MA., Elliott M., Suttorp M., Bogart L., et al. (2009). Prevalence of interstitial cystitis/painful bladder syndrome in the United States. Journal of Urology, 186, 540-544. • Celler, B. G., Lovell, N. H., & Basilakis, J. (2003). Using information technology to improve the management of chronic disease. MJA, 179, 242-246. • Chao, C.C., Yang, J.M., & Jen, W.Y. (2007). Determining technology trends and forecasts of RFID by a historical review and bibliometric analysis from 1991 to 2005. Technovation, 27 (5), 268-279.
References • Clemens, J. Q., Meenan, R. T., O’Keeffe-Rosetti, M. C., Gao, S. Y., & Calhoun, E. A. (2006). Medical costs and medication use in women with interstitial cystitis. J Urol, 175 Suppl, 94-95. • Curtis, D. W., Pino, E. J., Bailey, J. M., Shih, E. I., Waterman, J., et al. (2008) SMART- An integrated wireless system for monitoring unattended patients, J Am Med Inform Assoc, 15, 44-53. • Dell JR. (2003). Chronic pelvic pain of bladder origin: A focus on interstitial cystitis. Int J FertilWomens Med, 48, 154-62. • Delvaux, M., Ben Soussan, E., Laurent, V., Lerebours, E., & Gay, G. (2005). Clinical evaluation of the use of the M2A patency capsule system before a capsule endoscopy procedure, in patients with known or suspected intestinal stenosis. Endoscopy, 37(9), 801-807. • DeWitt DE. (1991). Dyspareunia. Tracing the cause. Postgrad Med, 89, 67-87. • Domdouzis, K., Kumar B. & Anumba, C. (2007). Radio-frequency identification (RFID) applications: a brief introduction. Advanced Engineering Informatics, 21 (4), 350-355. • Driscoll A., Teichman JM. (2001). How do patients with interstitial cystitis present? J Urol, 166, 2118-20. • Evans RJ. Treatment approaches for interstitial cystitis: Multimodality therapy. Rev Urol 2002;4:S16-S20.
References • Forrest, J. B. (2006). Epidemiology and quality of life. J Reprod Med, 51(3) Suppl, 227-233. • Hanno PM.(2011). AUA guideline for the diagnosis and treatment of IC/BPS. J Urol ,185,2162-70. • Heim LJ. (2001). Evaluation and differential diagnosis of dyspareunia. Am Fam Physician, 63, 1535-44. • Held, P. J., Hanno, P. M., Wein, A. J., Pauly, M. V., Cahn, M. A. (1990). Epidemiology of interstitial cystitis. In Interstitial Cystitis: Current Concepts. London. • Ito, T., Miki, M., & Yamada, T. (2000). Interstitial cystitis in Japan. BJU Int, 86(6), 634-637. • Izquierdo, R., Meyer, S., Starren, J., Goland R., Teresi, J., et al (2007). Detection and remediation of medically urgent situations using telemedicine case management for older patients with diabetes mellitus, Therapeutics & Clinical Risk Management, 3(3), 485-489. • Jones, P., Clarke-Hill, C. & Hillier, D. (2005). Radio frequency identification and food retailing in the UK. British Food Journal, 107 (6), 356-360. • Karkkainen, M. (2003). Increasing efficiency in the supply chain for short shelf life goods using RFID tagging. International Journal of Retail and Distribution Management , 31, 529-536.
References • Kellogg-Spadt S., Whitmore KE. (2006). Role of the female urologist/urogynecologist. In: Goldstein I, Meston CM, Davis SR, Traish AM, eds. Women’s sexual function and dysfunction: Study, diagnosis and treatment. Vol. 17. London: Taylor and Francis, 708-14. • Kim SI & Kim HS (2008) Effectiveness of mobile and internet intervention in patients with obese type 2 diabetes. International Journal of Medical Informatics 77, 399-404. • Kumar K.D., Karunamoorthy L., Roth H. & Mirnalinee T.T. (2005). Computers in manufacturing: Towards successful implementation of integrated automation system. Technovation, 25(5), 477-488. • Kumar, S. & Budin E.M. (2006). Prevention and management of product recalls in the processed food industry: a case study based on an exporter’s perspective. Technovation, 26 (5-6), 739-750. • Lailly, P, Van Jaarsveld, C. H. M., Potts, H. W. W. & Wardle, J. (2010) How are habits formed: Modeling habit formation in the real world, Eur J Soc Psychol, 40, 998-1009. • Lee, L.S., Fiedler K.D., & Smith, J.S. (2008). Radio frequency identification (RFID) implementation in the service sector: a customer-facing diffusion model. International Journal of Production Economics, 112 (2), 587-600. • Leppilahti M., Sairanen J., Tammela TL., Aaltomaa S., Lehtoranta K., et al. (2005). Finnish Interstitial Cystitis-Pelvic Pain Syndrome Study Group. Prevalence of clinically confirmed interstitial cystitis in women: A population based study in Finland. J Urol , 174, 581-3.
References • Liang X, Wang Q. et al. (2011) Effect of mobile phone intervention for diabetes on glycaemic control: a meta-analysis, Diabet Med 28, 455-463 • MettsJF. (2001). Interstitial cystitis: Urgency and frequency syndrome. Am Fam Physician, 64, 1199-206. • Meyer, H. J., Chansue, N., & Monticelli, F. (2006). Implantation of radio frequency identification device (RFID) microchip in disaster victim identification (DVI). Forensic Sci Int.,157(2-3), 168-171. • Michael, Y. L., Kawachi, I., Stampfer, M. J., Colditz, G. A., Curhan, G. C. (2000). Quality of life among women with interstitial cystitis. J Urol, 164(2), 423-427. • Michie S, Ashford S, et al. (2011) A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychology & Health 26(11):1479-98. • Michie S & Johnson M (2012) Theories and Techniques of Behaviour Change: Developing a Cumulative Science of Behaviour Change. Health Psychology Review 6(1), 1-6. • Nickel JC. (2003), Interstitial cystitis-An elusive clinical target? J Urol , 170, 816-817. • Nickel JC., Tripp D., Teal V., Propert KJ., Burks D., et al. (2007). Interstitial Cystitis Collaborative Trials Group. Sexual function is a determinant of poor quality of life for women with treatment refractory interstitial cystitis. J Urol , 177, 1832-6.
References • Ngai, E.W.T., Suk, F.F.C. & Lo, S.Y.Y. (2008). Development of an RFID-based sushi management system: the case of a conveyor-belt sushi restaurant. International Journal of Production Economics, 112 (2), 630-645. • Oravisto, K. J. (1975). Epidemiology of interstitial cystitis. Ann ChirGynaecolFenn, 64(2), 75-77. • Owens C, Farrand P, Darvill R, Emmens T, Hewis E, Aitken P (2011) Involving service users in intervention design: a participatory approach to developing a text-messaging intervention to reduce repetition of self-harm. Health Expect. 2011 Sep;14(3):285-95 • PadmadasSS., Stones RW., & Matthews Z. (2006). Dyspareunia and urinary sensory symptoms in India: Population-based study. J Sex Med, 3, 114-20. • Park, M. J., Kim, H. S., & Kim, K. S. ( 2009) Cellular phone and Internet-based individual intervention on blood pressure and obesity in obese patients with hypertension, Int J Med Inform, 78, 704-710. • Parkin et al. (2011) the fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010. British Journal of Cancer, 105, S77-S81. • Poon, T.C., Choy, K.L., Chow, Harry K.H., Lau, Henry C.W., Chan, Felix T.S., et al. (2009). A RFID case-based logistics resource management system for managing order-picking operations in warehouses. Expert Systems with Applications, 36, 8277-8301.
References • Porru D., Politano R., Gerardini M., Giliberto GL., & Stancati S., et al., (2004). Different clinical presentation of interstitial cystitis syndrome. IntUrogynecol J Pelvic Floor Dysfunct, 15, 198-202. • Qu X., Simpson L.T., & Stanfield P. (2010). A model for quantifying the value of RFID-enabled equipment tracking in hospitals, Adv. Eng. Informat. 25(1), 23-31. • Reicher, J., Reicher, D., & Reicher, M. (2007). Use of radio frequency identification (RFID) tags in bedside monitoring of endotracheal tube position. J ClinMonitComput., 21(3), 155-158. • Renney ML et al. (2012) Emergency department patients’ preferences for technology-based behavioral interventions. Annals of Emergency Medicine, 60(2), 218-227. • Rogers, A., Jones, E., & Oleynikov, D. (2007). Radio frequency identification (RFID) applied to surgical sponges. SurgEndosc., 21(7), 1235-1237. • Sehati, S., Fung, R. C. Y., & Nealon J. (2007) An Internet-enabled, ambulatory patient monitoring and advice syste,, J Telmedicine & Telcare, 13(Supp. 1) 59-62. • Steege JF., Ling FW. (1993). Dyspareunia. A special type of chronic pelvic pain. ObstetGynecolClin North Am, 20, 779-93. • Tajima, M. (2007). Strategic value of RFID in supply chain management. Journal of Purchasing & Supply Management, 13(4), 261-273. • Tan T.H., & Chang C.S. (2010). Development and Evaluation of an RFID-Based e-Restaurant System for Customer-Centric Service. Expert Systems with Applications 37(9), 6482-6492.
References • Tan T.H., Liu T.Y.,& Chang C.C. (2007). Development and evaluation of an RFID-based ubiquitous learning environment for outdoor learning. Interactive Learning Environments, 15(3), 253-269. • Tincello DG., & Walker AC. (2005). Interstitial cystitis in the UK: Results of a questionnaire survey of members of the Interstitial Cystitis Support Group. Eur J ObstetGynecolReprodBiol, 118, 91-5. • Tu Y.J., Zhou W., Piramuthu S. (2009) Identifying RFID-embedded objects in pervasive healthcare applications. Decision Support Systems, 46, 586-593. • Tzeng S.F., Chen W.H., and Pai F.Y (2008), Evaluating the business value of RFID: Evidence from five case studies, Int. J. Production Economics, 112, 601-613. • Webb TL, Joseph J, Yardley L, and Michie S (2010) Using the Internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res 12(1): e4. • Webster DC, Brennan T. (1995). Use and effectiveness of sexual selfcare strategies for interstitial cystitis. UrolNurs, 15, 14-22. • Wehbe SA., Whitmore K., & Kellogg-Spadt S. (2010). Urogenital Complaints and Female Sexual Dysfunction (Part 1). J Sex Med, 7, 1704-1713.
References • Wu, E. Q., Birnbaum, H., Mareva, M., Parece, A., Huang, Z., et al. (2006). Interstitial Cystitis: Cost, treatment and co-morbidities in an employed population. Pharmacoeconomics, 24(1), 55-65. • Xiao, Y., Shen, X., Sun, B. & Cai, L. (2006). Security and privacy in RFID and applications in telemedicine. IEEE Communications Magazine, 44 (4), 64-72. • Zaslau S., Riggs DR., Perlmutter AE., Jackson BJ.,& Osborne J. (2008). Sexual dysfunction in patients with painful bladder syndrome is age related and progressive. Can J Urol, 15, 4158-62.
Acknowledgements • This study was supported in part by Taichung Hospital (Grant no. CTU100-PC-002) and National Science Council of Taiwan (Grant no. NSC100-2410-H-166-007-MY3). • This study has been accepted for publication in International Journal of Urology (doi: 10.1111/iju.12336) • Co-authors: Ming-Huei Lee (李明輝),1,3Huei-Ching Wu (吳惠卿),2,3Departments of 1Management Information System and 2Healthcare Administration, Central Taiwan University of Science and Technology, 3Department of Urology, Feng Yuan Hospital, Ministry of Health and Welfare, Taichung