Download
1 / 32
320 likes | 465 Vues
Spinal Disorders. Rita Carey-Nita. Herniated Disks. Herniated Disks Characterized by pain & paresthesias Follow a nerve path Common ailment & patients often have more than one herniated disk Pathophysiology Disk moves out of normal anatomical position

E N D
Spinal Disorders Rita Carey-Nita
Herniated Disks • Herniated Disks • Characterized by pain & paresthesias • Follow a nerve path • Common ailment & patients often have more than one herniated disk • Pathophysiology • Disk moves out of normal anatomical position • The annulus fibrosus which is the tough outer ring tears • Allows the nucleus pulposus which is the soft inner portion to protrude out • Compresses the nerve root cause
Herniated Disks • Signs & Symptoms • Cervical Disks herniation • Pain & Muscle spasms in the neck • Decreases ROM due to pain • Hand & arm pain is unilateral • Pain follows the distribution of the spinal nerve root • Numbness or parethesia • Asymmetrical weakness and atrophy of specific muscle group • Indicators of significant nerve compression
Herniated Disks • Thoracic Herniation • Not common • Back pain is noted • No muscle weakness normally • Lumbar Herniation • Low back pain • Radiates down one leg • Paresthesia • Weakness • Visible limp on affected leg • Difficulty walking on heels or toes • Muscle spasms • LROM • Decreased or absent knee or ankle tendon reflex • If L5-S1 severely herniated incontinence occurs
Herniated Disks • Diagnostic Tests • MRI • If surgery performed previously MRI with and without contrast will be ordered to differentiated between herniation & scar tissue • Myelogram
Therapeutic Measures • Medical treatment includes bedrest for 1-2 days followed by gradual increase in activity • Physical Therapy • Gradual progressive course of exercise that strengthens the muscles to stabilize the spine • Ultrasound—ice—heat—deep massage can all help decrease muscle spasms & increase ROM • Proper body mechanics & strategies to avoid reinjury • Transcutaneous electrical nerve stimulator may be utilized
Therapeutic Measures • Traction • Noninvasive treatment of cervical herniations • Not done for lumbar herniations • Head is placed in halterlike device • Ropes & pulleys connect weight to gently pull head away from shoulders • Slight separation between vertebrae may allow the disc to return to proper position • If effective may be done at home as a prn treatment • If pain occurs traction is D/C
Medication • Muscle relaxants to decrease spasm which in turn decreases pain and increase ROM • Diazepam is effective relaxant but only used when other relaxants are ineffective because of its addictive properties • Acute spasm are protective • Chronic spasms cause tearing & scarring of muscles • Common side effect is drowsiness so need to use caution • NSAIDS • Used to reduce inflammation of nerve root caused by compression and irritation of nerve root • Educate pt • Not to use nonprescription while taking prescription NSAIDS • Report any GI upset because of risk for GI bleeding
Medication • Oral steroids • Short term treatment for severe inflammation that does not respond to other treatment • Taper dose over 1 week treatment is often prescribed • Diabetics need to monitor glucose which may elevate • Monitor for GI upset • Epidural injections • Mixture of steroid—anesthetic—long acting pain reliever • Injected into epidural space • Repeated every 3-4 months • Opiods are appropriate for short term treatment • Constipation—dependence—tolerance are all concerns with long-term use
Surgical Management • Laminectomy • Removal of the laminae • Relieves pressure or allows access for removal of herniated disk • Diskectomy • Removes entire disk • Usually done for cervical herniation • Spinal Fusion • Use bone graft to fuse 2 vertebrae together if unstable • Mobility of spine is lost • Corrects instability of spine with issues such as scoliosis or degenerative disorders or with diskectomy
Surgical Management • Herniated Cervical Disks • Diskectomy performed • Anterior or posterior approach with anterior preferred • Disk is replaced with bone or dense material • Bone harvested from iliac crest or cadaver • Spinal fusion is then performed limiting mobility in area of fusion
Herniated Lumbar Disks • Laminectomy performed resecting herniated portion of the disk • Remainder of disc is remains to provide cushion between intravertebral bodies • Posterior approach • 1-2 inch vertical incision with movement of muscles away from bone
Surgical Interventions • Laparoscopic technique • Surgery can be done through microscope • less invasive—less scarring—faster recovery—quicker discharge • PercutaneousDiskectomy • Insertion of large needle into the disk under local anesthesia with aspiration of herniated disk material • Not used on severely herniated disks • Laser Disk Surgery • May be used to disintegrate the herniated tissue
Complications • Hemmorhage • Always risk with any surgery • Not common in disk surgery • Monitor for bleeding at incision site • Monitor for respiratory distress • Monitor for airway obstruction with anterior cervical diskectomy • Nerve Root Damage • If severed during surgery patient loses motor & sensory fuction to the area served by that root • Can cause decrease use of extremity • Pain—weakness—paresthesia may result if damaged or scarring
Complications • Reherniation • Lumbar disk may reherniate • Can happen at any time after surgery • If it occurs within a few weeks to months of surgery another microdiskectomy will be performed • Cervical reherniation does not occur because the disk is removed • Herniation of another disk • Fusion of the cervical spine results in loss of movement at that area which places stress on disk above & below increasing the risk of them herniating • Especially a concern if degenerative disease is present • Prevention includes ROM exercises
Preoperative & Postoperative Care • Preoperative teaching should include: • Proper body alignment • Teach log rolling • Postoperative care • Routine assessment • Neurovascular assessment • Pain assessment • Surgical site assessment • Monitor I&O
Spinal Stenosis • Spinal stenosispathophysiology • Spinal canal compresses on spinal cord • Arthritis is major cause • Facet joints become inflamed & enlarged • Signs & Symptoms • Pain & weakness • Cervical stenosis • Therapeutic Intervention • Laminectomy • Rehabilitation postoperatively before discharge to home with older patients
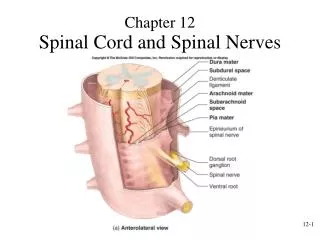
Spinal Cord Injury • Pathophysiology • Damage to spinal cord that interferes with sensory and motor function • May include: • Bruising—tearing—cutting—edema—bleeding of cord • May be external force or fragments of fractured bone • Causes • MVA • Sports injuries • Falls • Voilence
Spinal Cord Injury • Classified by location and degree of damage to the cord • Complete spinal cord injury results in complete loss of motor and sensory function below the level of the injury • Incomplete spinal cord injury results in some function remaining • Cervical & lumbar more common injury than thoracic & sacral
Spinal Cord Injury • Cervical Signs & Symptoms • Affect all four extremities • Quadriplegia • Quadriparesis • paralysis—paresthesias—impaired respirations—loss of bowel & bladder control • C3 or above usually fatal injury • C4 –C5 injury may require ventilator support
Spinal Cord Injury • Thoracic & Lumbar Signs & Symptoms • Affects legs • Paraplegia • Paraparesis • Loss bowel & bladder function—paralysis—parathesia • Sacral Signs & Symptoms • Loss of bowel and bladder function • Impaired foot function
Spinal Shock • Injury affects ANS • Disrupts the Sympathetic portion • Causes: • Vasodilation • Hypotension • Bradycardia • Hypothermia with inability to control temp • Urinary & feces retention • Loss of motor & sensory function below the injury • May last a week to weeks
Complications • Infection • Pneumonia • Urinary tract infection • Deep vein thrombosis • Lack of movement in legs • Orthostatic hypotension • Loss of motor function affects venous return • Impaired vasoconstriction • Skin breakdown • Diligent care & repositioning necessary
Complications • Renal complications • UTI’s & urinary reflux cause permanent kidney damage • Depression & Substance Abuse • Higher incidence which affect self-care • Counseling & support groups may help
Complications • Autonomic Dysreflexia • Life-threatening complication for injuries above T6 level • Impaired balance between SNS & PNS • Stimuli below the injury causes activation of SNS • PNS can not counteract SNS because message can not be sent below the level of the injury • Most common cause is bladder distention • Others include: • Bowel impaction—UTI—ingrown toenail—pressure ulcers—pain—labor • Stimulation of SNS causes: • Cool pale skin—gooseflesh—vasoconstriction below the injury • Hypertension • PNS response causes: • Vasodilation—headache—nasal congestion—flushing—diaphoresis—bradycardia above the injury
Diagnostic Tests • Xray • Shows fracture or displacement of vertebrae • CT scan • Identifies fracture • MRI • Identifies lesions within cord
Therapeutic Interventions Therapeutic Interventions • Immobilized until assessed • Especially if spinal cord injury suspected • Bowel & bladder training • Nutrition/ Diet • Activity • Rehabilitation • Prevention of skin breakdown • Prevention of dysreflexia • Sexual counseling
Emergency Management • Monitor vitals • Maintain airway • Keep immobilized • May need intubation & mechanical ventilation • Fluid replacement to help hypotension • Vasopressor if fluid alone ineffective • Intravenous Methylprednisolone may be administered
Respiratory Management • Respiratory impairment with injury above C4-C5 • Tracheostomy & continuous ventilation may be necessary • Phrenic nerve stimulator may be indicated if nerve paralyzed • Causes of respiratory compromise • Edema of cord can compromise respiratory function • Fatigue of accessory muscles • May require mechanical ventilation initially but as edema recedes they can be weaned
Gastrointestinal & Genitourinary Management Gastrointestinal Management • Absence of bowel sounds common finding • Need bowel function before oral or enteral feeding started • May require hyperalimentation to meet the metabolic needs of the body Genitourinary Management • Indwelling catheter • Bladder management program Immobilization • Cervical spine may be immobilized with skeletal traction
Surgical Management • Goal • Stabilize the bone elements of spine • Relieve pressure on spinal cord • May or may not improve function • Allows for early mobilization decreasing risk for complications • Quickens the transition into rehabilitation • May have postoperatively • Cervical—halo brace • Thoracic & Lumbar—implantation of rods • May have rigid brace or body cast as well
Nursing Care for Spinal Cord Injury • Frequent neurological assessment • Frequent respiratory assessment • Assess for evidence of complication • Autonomic dysreflexia • Monitor skin integrity • Monitor for bowel or bladder elimination issues • Signs of UTI • Impaction • Note any self-care deficits • Note any signs of depression or anxiety