Download
1 / 30
360 likes | 840 Vues
Chronic Fatigue Syndrome. Ashton Jeppesen. WHY Chronic Fatigue??. I got MONO when I was 19, and still suffer from chronic fatigue Thought it would be interesting to find out current research. How set up an exercise plan. Definition Epidemiology Symptoms Diagnosis Complications

E N D
Chronic Fatigue Syndrome Ashton Jeppesen
WHY Chronic Fatigue?? • I got MONO when I was 19, and still suffer from chronic fatigue • Thought it would be interesting to find out current research. • How set up an exercise plan
Definition • Epidemiology • Symptoms • Diagnosis • Complications • Treatments • Effects of Disease & Medicine on Exercise • Effects of Bout of exercise on Patient vs. Effects of Training • Exercise Prescription • Summary OVERVIEW
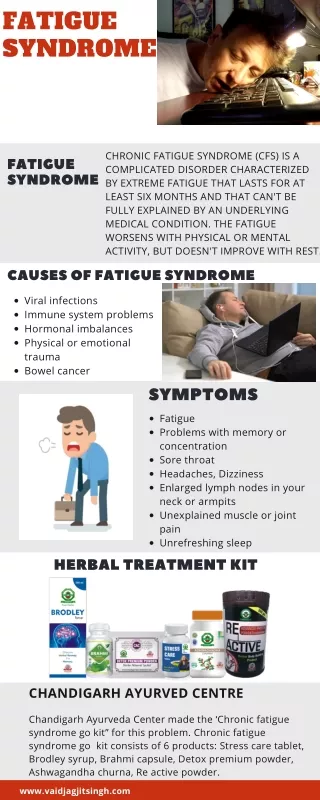
Define: Chronic Fatigue Syndrome CFS • Also known as Chronic Fatigue and Immune Dysfunction Syndrome (CFIDS) • CFS is a puzzling & complex idiopathic condition defined only by symptoms • Persistent debilitating fatigue, not relieved by rest, and not accounted by any specific identified medical or psychiatric conditions
Definition Continued… Criteria for CFS (Chronic Fatigue Syndrome) • Severe chronic fatigue lasting 6 months • 4 or more of the following symptoms • Substantial impairment in short-term memory or concentration • Sore throat • Tender lymph nodes • Muscle pain • Multi-joint pain without swelling or redness • Headaches of a new type, patter, or severity • Un-refreshing sleep • Post-exertional malaise lasting at least 24 hrs.
Incidence or Prevalence Prevalence is between 400 to 2,500 adults per 100,00 population Just under 1 million people more common in women, white majority, middle class Recently, show CFS is higher in lower socioeconomic status and minority cultural or ethic groups CFS is associated with social strain, negative aspects of social support, physical inactivity, anxiety & depression.
Causes??? Causes of CFS is still unknown but possible causes include: Viral infection (MONO) Immunologic dysfunction Abnormal hypothalamic-pituitary-adrenal (HPA) axis activity Neurally mediated hypotension Nutritional deficiency Profound psychological stress
On-going fatigue-not relieved by rest • Headaches • Sleep disturbance • Muscle pain • Frequent sore throat • Painful lymph nodes • Difficulty concentration & memory • Low-grade fever • Aches Symptoms inhibit day to day activities Symptoms
Diagnosis & Test According to the Centers for Disease Control (CDC) If someone has substantial reduction in previous levels of occupational, educational, social, and or personal activities. If there is an occurrence of 4 or more of the following symptoms: impairment in short-term memory sore throat, tender lymph nodes, muscle pain, multi-joint pain, headaches, sleep is not refreshing, post-exertional malaise (more than 24hrs)
Diagnosis………. A physician must exclude all other conditions that may precipitate similar symptoms To exclude all conditions, a person with CFS must endure countless laboratory test and procedures ***Thus a fitness professional must appreciate the long, exhausting, and frustrating journey their client has to take before receiving the diagnosis of CFS
Diagnosis & Test Since the diagnosis of CFS is based solely on symptoms, there are no recommended specific lab test. Lab test should be focused on confirming or excluding other possible conditions ***White blood cell count……any monocytes or granulocytes ?
Typical Treatments Pharmacological therapy Sleep hygiene Dietary management & nutritional supplements Activity management Cognitive Behavioral Therapy/Graded Exercise Alternative approaches
2 COMMON TREATMENTS (for exercise) 1.Cognitive-behavioral treatment 2. Graded Exercise Therapy Treatments
Treatments Cognitive Behavioral Therapy (CBT) :is a psychotherapeutic approach: a talking therapy. CBT aims to solve problems concerning dysfunctional emotions, behaviors and cognitions through a goal-oriented, systematic procedure in the present. FEAR OF EXERCISE Graded Exercise Therapy : improving physiological exercise capacity and exercise tolerance by gradually increasing exercise intensity and duration.
Graded Exercise Therapy (GET) Main goal is to 1st increase duration and 2nd to increase intensity. Duration Patients need to start at a low baseline for 2 weeks, exercising at least for 5 days Then incrementally increase daily exercise on duration until they are doing 30 min of exercise for 5 days Can be done in sessions of 10 to 15 mins
Graded Exercise Therapy Intensity Once 30 minutes of daily exercise is achieved, intensity should be increased. 10-20%, but no more than 20% weekly. If patient develops symptoms as a response to increased intensity, they should KEEP exercising at that level, rather than stop The body with start to adapt and the symptoms should subside Let your patient/client chose what kind of exercise and dosage they will preform because they will be more likely to continue exercising
One study from Journal of Pediatrics and Child Health, 2009 showed: • GET had a significant effect in aerobic capacity on CFS • Increase in exercise duration by 18% • Also increase in time to fatigue, exercise intensity (METs) and peak oxygen uptake • Upper body muscular strength and endurance through a 70% increase in # of pushups Overall concluded that GET is effective in improving quality of life and depressive feelings Research
Educating Clients Providing information about home exercise programs, their illness & treatment, is considered an important part of the therapy process. Early research has shown that if patients recognize the benefits from exercise ,on their chronic disease, than they are more likely to continue physical activity. In the general population, ½ of all who participate in supervised exercise programs stop within 3-6 months…
Common Effects of Disease on Ability to Exercise • Post-exertion malaise /more than 24hrs • Musculoskeletal pain- in vigorous exercise • Worsening symptoms • So, it is important for patients to learn how to estimate their current physical capability, prior to exercise. • When exercise, patients need lots of breaks, with the lengths of the breaks equaling duration of activity • Patients can’t just work out when they want to work out. They need to be in the “RIGHT” mind!
Acute Effects of Chronic Fatigue on Exercise Higher RPE at every work load compared to healthy controls Slower hear rate acceleration as workloads increase Some may have 10 to 50% lower maximal power output compared to controls Expect to experience an increase in symptoms after completion of a single bout of exercise
Chronic Effects of Exercise with CFS clients • One study showed that those who participated in a low impact aerobic dance session 2x per week (20 weeks) had significant decrease in exercise induced pain. • In the long run, exercise programs have shown to improve pain, fatigue, and/or anxiety/depression. • Overall it was not shown improvements with strength, but more the ability to tolerate pain without symptoms getting worse!! • Prevent deconditioning
Commonly used Exercise tests • Submaximal test using the Balke & Naugton Treadmill protocols • Cycle ergometer protocols • Start slow, go slow • Primary concern is an adequate warm-up and tolerable rate of increase to minimize premature local muscle failure and fatigue • 6 min walk test- better used as functional test, rather than measurement of cardiorespiratory fitness.
Exercise Testing Incremental exercise testing with monitoring of standard cardiovascular & ventilatory responses. electrocardiogram, blood pressure, heart rate monitor, respiratory gas exchange and ventilation may be indicated as a screening test for individuals whose diagnosis is not yet established. Remember , individuals with long-standing symptoms are very likely to have a low level exercise activity & have undergone significant DECONDITIONING.
Exercise Testing • Work rates will therefore usually start out low relative to standard protocol. Based on predicted age, size, and gender. • Work rates below 2 METs and increase .5 to 1 MET per stage. NOTE • Testing should be scheduled for a day when the client does not have other activities scheduled
Exercise Goals/Programming Goals 1st- prevent further deconditioning Resist the temptation to adopt a traditional method of training aimed at aerobic capacity Instead focus on modest goals for preventing deconditioning Focus on increasing duration not intensity. Programming RPE should be the primary goal to determine exercise intensity of the client Aerobic exercise should be one that is familiar to them. For strength training stay away from delayed onset muscle soreness (DOMS). Eccentric exercises!!
Therapeutic Range Maximal Tolerated Dose Response Dose Pharmacotherapy model
Summary &Conclusion • CFS is defined by symptoms, therefore there isn’t any diagnosis test • Chronic Fatigue is fatigue lasting at least 6 months • Exercise is one of the common treatments for CFS • The goals for exercise are 1st duration 2nd intensity • RPE is the primary key for intensity • When testing CF patients remember their workloads are going to be lower than the norms and to increase slower than normal • Encourage client to not stop if symptoms resume, to just continue to exercise and the body will adapt • BE PATIENT
References Bailey, S. P. T. ,. D. ,. F. (2011). Exercise as a treatment for chronic fatigue syndrome. ACSM Health & Fitness Journal, 15(1), 20-25. Clark, L., & White, P. (2005). The role of deconditioning and therapeutic exercise in chronic fatigue syndrome (CFS). Journal Of Mental Health, 14(3), 237-252 doi:10.1080/09638230500136308 Darcy, P., Napora, L., DeMarco, C., & Remsber, C. (2002). Acsm's resources for clinical exercise physiology. (1 ed., pp. 111-120). Baltimore: Lippincott Williams & Wilkins. Durstine, J. L., Moore, G. E., Painter, P. L., & Roberts, S. O. (2009). Acsm's exercise management for persons with chronic diseases and disabilities. (3rd ed., pp. 233-237). Champaign, IL: Human Kinetics. Gordon, B. A., Knapman, L. M., & Lubitz, L. (2010). Graduated exercise training and progressive resistance training in adolescents with chronic fatigue syndrome: a randomized controlled pilot study. Clinical Rehabilitation, 24(12), 1072-1079. doi:10.1177/0269215510371429 Gordon, B. and Lubitz, L. (2009), Promising outcomes of an adolescent chronic fatigue syndrome inpatient programme. Journal of Paediatrics and Child Health, 45: 286–290. doi: 10.1111/j.1440-1754.2009.01493.x Nijs, J., Paul, L., & Wallman, K. (2008). Chronic fatigue syndrome: an approach combining self- management with graded exercise to avoid exacerbations. Journal Of Rehabilitation Medicine: Official Journal Of The UEMS European Board Of Physical And Rehabilitation Medicine, 40(4), 241-247. Skinner S., J. (2005). Exercise testing and exercise prescription for special cases. (3rd ed. ed., pp. 188- 199). Baltimore: Lippincott Williams & Wilkins.