Download
1 / 1
10 likes | 168 Vues
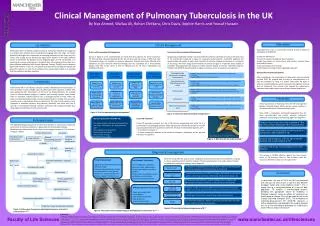
Clinical Management of Pulmonary Tuberculosis in the UK. Adherence. Introduction. Clinical Management. By Naz Ahmed, Wallaa Ali, Rohan Chitkara , Chris Davis, Sophie Harris and Yousuf Hussain.

E N D
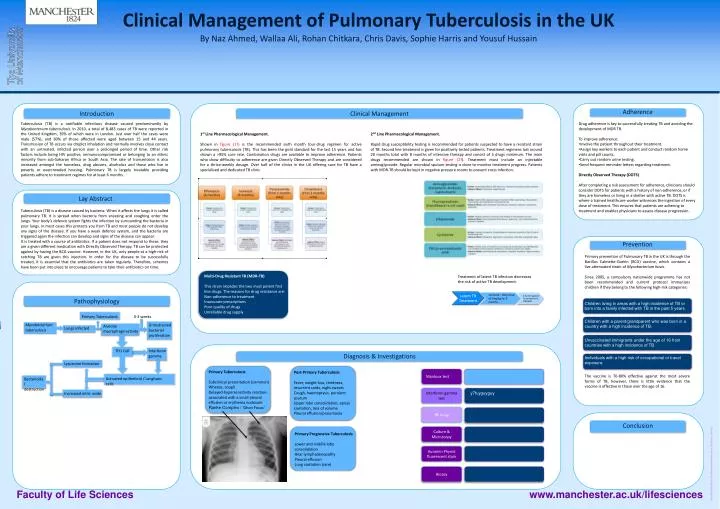
Clinical Management of Pulmonary Tuberculosis in the UK Adherence Introduction Clinical Management By Naz Ahmed, Wallaa Ali, RohanChitkara, Chris Davis, Sophie Harris and Yousuf Hussain Tuberculosis (TB) is a notifiable infectious disease caused predominantly by Mycobacterium tuberculosis. In 2010, a total of 8,483 cases of TB were reported in the United Kingdom, 39% of which were in London. Just over half the cases were male (57%), and 60% of those affected were aged between 15 and 44 years. Transmission of TB occurs via droplet inhalation and normally involves close contact with an untreated, infected person over a prolonged period of time. Other risk factors include being HIV positive, immunocompromised or belonging to an ethnic minority from sub-Saharan Africa or South Asia. The rate of transmission is also increased amongst the homeless, drug abusers, alcoholics and those who live in poverty or overcrowded housing. Pulmonary TB is largely treatable providing patients adhere to treatment regimes for at least 6 months. • Drug adherence is key to successfully treating TB and avoiding the development of MDR TB. • To improve adherence: • Involve the patient throughout their treatment. • Assign key workers to each patient and conduct random home visits and pill counts. • Carry out random urine testing. • Send frequent reminder letters regarding treatment. • Directly Observed Therapy (DOTS) • After completing a risk assessment for adherence, clinicians should consider DOTS for patients with a history of non-adherence, or if they are homeless or living in a shelter with active TB. DOTS is where a trained healthcare worker witnesses the ingestion of every dose of treatment. This ensures that patients are adhering to treatment and enables physicians to assess disease progression. 1st Line Pharmacological Management. Shown in figure (1?) is the recommended sixth month four-drug regimen for active pulmonary tuberculosis (TB). This has been the gold standard for the last 15 years and has shown a >95% cure rate. Combination drugs are available to improve adherence. Patients who show difficulty to adherence are given Directly Observed Therapy and are considered for a thrice-weekly dosage. Over half of the clinics in the UK offering care for TB have a specialised and dedicated TB clinic. 2nd Line Pharmacological Management. Rapid drug susceptibility testing is recommended for patients suspected to have a resistant strain of TB. Second line treatment is given for positively tested patients. Treatment regimens last around 20 months total with 8 months of intensive therapy and consist of 5 drugs minimum. The main drugs recommended are shown in figure (2?). Treatment must include an injectableaminoglycoside. Regular microbial sputum testing is done to monitor treatment progress. Patients with MDR-TB should be kept in negative pressure rooms to prevent cross infection. Lay Abstract Tuberculosis (TB) is a disease caused by bacteria. When it affects the lungs it is called pulmonary TB. It is spread when bacteria from sneezing and coughing enter the lungs. Your body’s defence system fights the infection by surrounding the bacteriain your lungs. In most cases this protects you from TB and most people do not develop any signs of the disease. If you have a weak defence system, and the bacteria are triggered again the infection can develop and signs of the disease can appear. It is treated with a course of antibiotics. If a patient does not respond to these, they are a given different medication with Directly Observed Therapy. TB can be protected against by having the BCG vaccine. However, in the UK, only people at a high-risk of catching TB are given this injection. In order for the disease to be successfully treated, it is essential that the antibiotics are taken regularly. Therefore, schemes have been put into place to encourage patients to take their antibiotics on time. Prevention Primary prevention of Pulmonary TB in the UK is through the Bacillus Calmette-Guérin (BCG) vaccine, which contains a live attenuated strain of Mycobacterium bovis. Since 2005, a compulsory nationwide programme has not been recommended and current protocol immunises children if they belong to the following high-risk categories: Fully susceptible all 1st line drugs Mono-resistant Resistant to single 1st line drug Multi-resistant Resistant to Isoniazid and Rifampicin Poly-resistant Resistant to 2 or more 1st line drugs Extensively Drug Resistant (X-DR TB) Failed MDR-TB treatment,resistance to fluroquinolone, amino glycoside and one 2nd line drug • Multi-Drug Resistant TB (MDR-TB) • This strain impedes the two most potent first line drugs. The reasons for drug resistance are: • Non-adherence to treatment • Inaccurate prescriptions • Poor quality of drugs • Unreliable drug supply Treatment of latent TB infection decreases the risk of active TB development. Effectiveness of Treatment Pathophysiology • Isoniazid – daily dose of 5mg/kg for 9 months. Children living in areas with a high incidence of TB or born into a family infected with TB in the past 5 years. • 3 month regimen • of isoniazid and rifampicin Primary Tuberculosis 0-3 weeks Mycobacterium tuberculosis Lungs infected Children with a parent/grandparent who was born in a country with a high incidence of TB. Unrestrained bacterial proliferation Alveolar macrophage activity Lungs infected Mycobacterium tuberculosis Primary Tuberculosis • Alveolar macrophage • activity Unvaccinated immigrants under the age of 16 from countries with a high incidence of TB. 0-3 weeks Unrestrained bacterial proliferation >3 weeks TH1 Cell Interferon gamma Diagnosis & Investigations Individuals with a high risk of occupational or travel exposure. TH1 Cell Lysosome formation • Interferongamma • Primary Tuberculosis • Subclinical presentation (common) • Wheeze, cough • Delayed-hypersensitivity reaction-associated with a small pleural effusion or erythemanodosum • Ranke Complex / 'GhonFocus’ • Post-Primary Tuberculosis • Fever, weight loss, tiredness, recurrent colds, night sweats • Cough, haemoptysis, purulent sputum • Upper lobe consolidation, apical cavitation, loss of volume • Pleural effusion/pneumonia The vaccine is 70-80% effective against the most severe forms of TB, however, there is little evidence that the vaccine is effective in those over the age of 16. Mantoux test Activated epithelioid / Langhans cells Bactericidal destruction Interferon gamma test y7fuyguyguy Increased nitric oxide Bactericidal destruction • Activated • epithelioid/ Langhans cells Lysosome formation PA X-ray Antimicrobial immunity Hypersensitivity reaction Increased nitric oxide Conclusion Culture & Microscopy • Primary Progressive Tuberculosis • Lower and middle lobe consolidation • Hilarlymphadenopathy • Pleural effusion • Lung cavitation (rare) Caseating granuloma ‘Ghon focus’ Latent Tuberculosis Post-Primary Tuberculosis AuraminPhynol fluorescent stain Reactivation/Reinfection Progressive tissue damage with cavitation Healed lesion Primary Progressive Tuberculosis Biopsy Faculty of Life Sciences www.manchester.ac.uk/lifesciences