Download
1 / 42
420 likes | 578 Vues
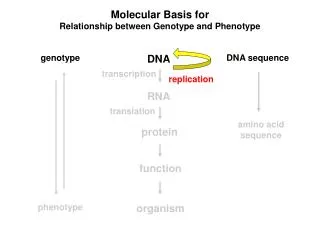
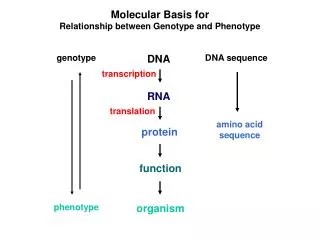
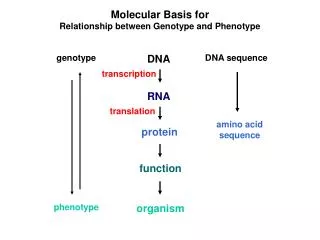
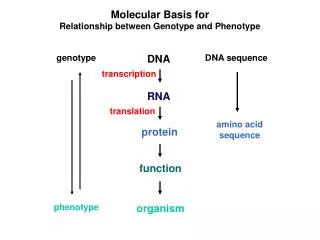
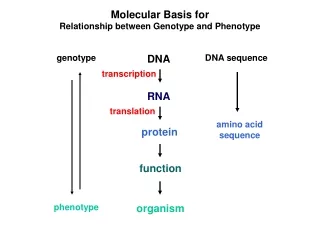
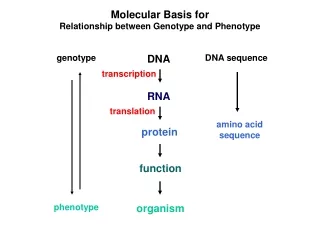
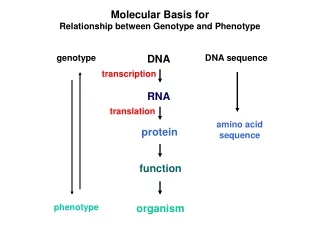
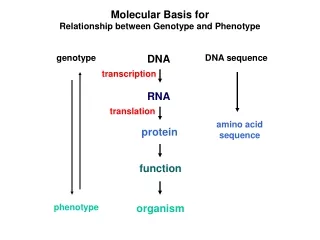
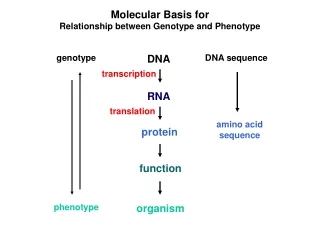
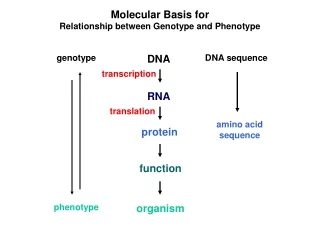
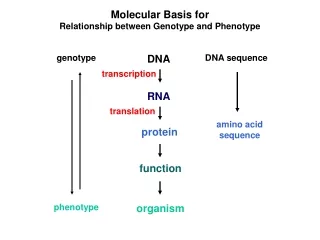
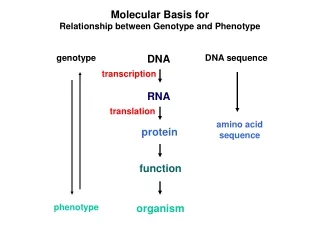
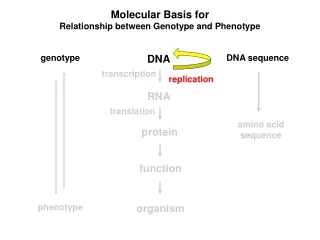
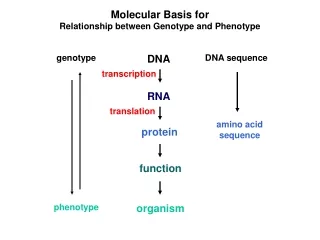
The Molecular Phenotype of Heart Allograft Biopsies. Mario C Deng Associate Professor of Medicine Director of Cardiac Transplantation Research Center for Advanced Cardiac Care Department of Medicine Columbia University USA. modern medicine & immortality.

E N D
The Molecular Phenotype of Heart Allograft Biopsies Mario C Deng Associate Professor of Medicine Director of Cardiac Transplantation Research Center for Advanced Cardiac Care Department of Medicine Columbia University USA
modern medicine & immortality New York Times Magazine Jan 30, 2000
heart transplant milestones • Animal Htx (Shumway) • Electrical VAD (Portner) (1959) • First human Htx (Barnard) • Endomyocardial Biopsy (Caves) (1967) (1973) • Copeland re-Htx (Copeland) (1974) • Human HLtx (Reitz) (1981) • Baby Htx (Bailey) (1984) • H. Genome (Lander) (2000) • Allomap (Deng) • Steroids • ATGAM • Fk506 • Sirolimus (2005) • Azathioprin • Neoral • MMF • CsA • Chemogenomics • OKT3 • Daclizumab 1975 1985 1995 2005 1965 2009
heart transplant survival by era Survival (%) ISHLT Taylor D et al. J Heart Lung Transplant 2008;27: 937-983
heart transplant cause of death ISHLT Taylor D et al. J Heart Lung Transplant 2008;27: 937-983
allograft rejection Recipient immune response T-cell activating signals #1 T-cell receptor #2 CD28 #2a CD40L #3 IL2, IL15 etc Bone marrow thymus TCR CD3+ T-cell monocyte B-cell Allo Ag allo MHC Allo Ag self MHC spleen lymphnode CD8+ CD4+ allo APC self APC rejection CD4+Th1 CD8+ Cytotox CD4+/45RO+ Cardiac allograft tolerance CD4+/25+ CD8+ suppr CD8+28- suppr CD4+Th2
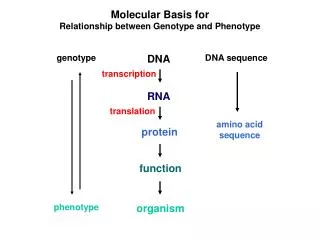
systems biology strategy Rejection Quiescence phenome metabolome proteome transcriptome genome
Recipient immune response Rejection Quiescence T-cell activating signals #1 T-cell receptor #2 CD28 #2a CD40L #3 IL2, IL15 etc phenome TCR metabolome CD3+ T-cell monocyte B-cell Allo Ag allo MHC Allo Ag self MHC proteome CD8+ CD4+ transcriptome allo APC self APC rejection CD4+Th1 CD8+ Cytotox CD4+/45RO+ genome Cardiac allograft tolerance CD4+/25+ CD8+ suppr CD8+28- suppr CD4+Th2 allograft rejection
endomyocardial biopsy mild severe status quo monitoring • invasive & complication-prone • late-stage cellular rejection diagnosis • insensitive for humoral rejection • significant variability • no insight into molecular mechanisms • resource-intense
rejection grading • no rejection • A, focal infiltrate without necrosis • B, diffuse sparse infiltrate w/o necrosis • one focus aggressive infiltration/focal myocyte damage • A, multifocal aggr infiltr or myoc damage • B, diffuse inflamm process with necrosis • diffuse, necrosis, edema, hemorrhage • 0 R • 1 R • 2 R • 3 R • 0 • 1 • 2 • 3 • 4 AMR Quilty Billingham ME et al. J Heart Lung Transplant 1990;9:587 Stewart S et al. J Heart Lung Transplant 2005;24:1710
current standard of literature • Nielsen H., F.B. Sorensen and B. Nielsen et al., Reproducibility of the acute rejection diagnosis in human cardiac allografts. The Stanford Classification and the International Grading System, J Heart Lung Transplant 12 (1993), pp. 239–243 • Fishbein M.C., G. Bell and M.A. Lones et al., Grade 2 cellular heart rejection does it exist?, J Heart Lung Transplant 13 (1994), pp. 1051–1057 • Winters G.L., E. Loh and F.J. Schoen, Natural history of focal moderate cardiac allograft rejection. Is treatment warranted?, Circulation 91 (1995), pp. 1975–1980 • Milano A., A.L. Caforio and U. Livi et al., Evolution of focal moderate rejection of the cardiac allograft, J Heart Lung Transplant 15 (1996), pp. 456–460 • Brunner-La Rocca H.P., G. Sutsch, J. Schneider, F. Follath and W. Kiowski, Natural course of moderate cardiac allograft rejection early and late after transplantation, Circulation 94 (1996), pp. 1334–1338 • Mills R.N., D.C. Naftel and J.K. Kirklin et al., Heart transplant rejection with hemodynamic compromise a multiinstitutional study of the role of endomyocardial cellular infiltrate. Cardiac Transplant Research Database, J Heart Lung Transplant 16 (1997), pp. 813–821 • Winters G.L., B.M. McManus and Rapamycin Cardiac Rejection Treatment Trial Pathologists, Consistencies and controversies in the application of the ISHLT working formulation for cardiac transplant biopsy specimens, J Heart Lung Transplant 17 (1998), p. 754 • Rodriguez E.R. and International Society for Heart and Lung Transplantation, The pathology of heart transplant biopsy specimens revisiting the 1990 ISHLT working formulation, J Heart Lung Transplant 22 (2003), pp. 3–15 Marboe CC, Billingham M, ... Berry G. JHLT 2005;24:S219
Recipient immune response Rejection Quiescence T-cell activating signals #1 T-cell receptor #2 CD28 #2a CD40L #3 IL2, IL15 etc phenome TCR metabolome CD3+ T-cell monocyte B-cell Allo Ag allo MHC Allo Ag self MHC proteome CD8+ CD4+ transcriptome allo APC self APC rejection CD4+Th1 CD8+ Cytotox CD4+/45RO+ genome Cardiac allograft tolerance CD4+/25+ CD8+ suppr CD8+28- suppr CD4+Th2 allograft rejection
intragraft cytokine expression Alvarez CM et al. Clin Transplant 2001;15:228
intragraft cytokine expression Alvarez CM et al. Clin Transplant 2001;15:228
correlation of IL6 with rejection Author Year No Time Method Result Zhao 1994 21 early RT-PCR IL6, TGFß+ Van Hoffen 1996 40 first mo‘s ISH/IHC IL6,8,9,10+ Baan 1996 16 < 12 mo RT-PCR IL4,IL6+ Kimball 1996 62 < 30d ELISA IL6,8+ Van Besouw 1997 85 > 1 y GIL-ELISA IL6+ TxV
no correlation of IL6 with rejection Author Year No Time Method Result Ruan 1992 113 ? IHC IL6-,IL2+,IFN+ Fyfe 1993 40 var ELISA IL4, IL6,TNF- Van Besouw 1995 49 < 90d culture IL6-,IL4-,IL2,IFN+ Grant 1996 259 <2y ELISA IL6- Lagoo 1996 328 < 8 wk RT-PCR IL6- Grant 1996 187 <2y RT-PC/ELISA IL6-,IL2+ George 1997 484 < 8 wk ELISA IL6,IL8,TNF- Deng 1998 115 <3mo ELISA IL6- Salom 1998 22 early IHC IL6-, IL1, TNF+
systems biology strategy Phenotype 1 Phenotype 2 phenome/physiome metabolome proteome 0 bottom-to-top top-to-bottom transcriptome genome
pathogenesis-based transcript sets ...We used mouse transplants to annotate pathogenesis-based transcript sets (PBTs) that reflect major biologic events in allograft rejection—cytotoxic T-cell infiltration, interferon-γ effects and parenchymal deterioration. We examined the relationship between PBT expression, histopathologic lesions and clinical diagnoses in 143 consecutive human kidney transplant biopsies for cause. PBTs correlated strongly with one another, indicating that transcriptome disturbances in renal transplants have a stereotyped internal structure. This disturbance was continuous, not dichotomous, across rejection and nonrejection. PBTs correlated with histopathologic lesions and were the highest in biopsies with clinically apparent rejection episodes. Surprisingly, antibody-mediated rejection had changes similar to T-cell mediated rejection. Biopsies lacking PBT disturbances did not have rejection. PBTs suggested that some current Banff histopathology criteria are unreliable, particularly at the cut-off between borderline and rejection...many transcriptome changes previously described in rejection are features of a large-scale disturbance characteristic of rejection but occurring at lower levels in many forms of injury. PBTs represent a quantitative measure of the inflammatory disturbances in organ transplants, and a new window on the mechanisms of these changes. Mueller TF et al. Am J Transplant 2007;7:1
endomycardial array & rejection Karason K et al. BMC Cardiov Dis 2006;6:29
endomycardial array & rejection Karason K et al. BMC Cardiov Dis 2006;6:29
endomycardial array & rejection Karason K et al. BMC Cardiov Dis 2006;6:29
endomycardial array & rejection Karason K et al. BMC Cardiov Dis 2006;6:29
endomycardial array & rejection …Methods: Endomyocardial tissue samples and serum were obtained in connection with clinical biopsies ... Endomyocardial RNA,..were analysed with DNA microarray. Genes showing up-regulation during rejection followed by normalization after the rejection episode were evaluated further with real-time RT-PCR…ELISA was performed to investigate whether change in gene-regulation during graft rejection was reflected in altered concentrations of the encoded protein in serum…Results…CCL9 was significantly upregulated during rejection (p < 0.05)…There were no changes in CXCL9 and CXCL10 serum concentrations during cardiac rejection…Conclusion: We conclude, that despite a distinct up-regulation of CXCL9 mRNA in human hearts during cardiac allograft rejection, this was not reflected in the serum levels of the encoded protein. Thus, in contrast to previous suggestions, serum CXCL9 does not appear to be a promising serum biomarker for cardiac allograft rejection. The lack of success in the identification of cardiac rejection biomarkers in the current study indicates that expression profiling of immunological active cells of the heart recipient may be a better way to identify cardiac rejection biomarkers. Karason K et al. BMC Cardiov Dis 2006;6:29
intragraft & PBL expression …Our results demonstrate that PBL gene expression profiles in acute rejection are distinctly different from those of normal controls and from patients with well-functioning transplants. Therefore, acute rejection does influence the gene expression profile of the circulating lymphocyte pool. Moreover, despite the fact that surprisingly we found very little common gene expression between PBLs and kidney biopsies, we did identify a large number of lymphocyte-specific genes in the kidney tissue. One interpretation is that there are compartment-specific differences between the PBLs in the circulation and the subset of lymphocytes that are activated and recruited to the transplant kidney during acute rejection. ..these results…may explain the failure of more than a decade of work testing PBLs for an array of activation antigens based on findings in rejecting allografts and other immune models…It is possible that the gene expression profile of the PBLs represents the adequacy of immunosuppression such that the rejecting patients reflect the profile of inadequate immunosuppression as compared with the PBLs sampled from patients with well-functioning transplants... there is a distinct gene expression profile in the PBL pool that correlates with acute rejection and immunosuppression. If these results can be confirmed in a large, prospective trial it would support the use of such profiles as a minimally invasive monitoring strategy for the immunological status of the graft and support the potential of using them to monitor the adequacy of immunosuppression… Flechner SM et al. Am J Transplant 2004;4:1475
current standard of care …the variability in the grading of heart transplant biopsies suggests the biopsy itself may not be a true gold standard against which all subsequent tests should be compared; this has clear implications for the evaluation of any new molecular diagnostic test if the only end-point is comparison with biopsy grade. Multifactorial end-points combining clinical, hemodynamic and biopsy data would provide a better standard. Indeed, the correlation of these multiple factors and peripheral blood gene expression with biopsy histology may provide a basis for further refining of the biopsy grading system by providing insight into the histologic features that best correlate with immunologic status and clinical outcomes. Marboe CC, Billingham M, ... Berry G. JHLT 2005;24:S219
networked alloimmunity • detection of cytokine transcripts does not imply protein • detection of cytokine protein does not imply function • function may vary in different contexts • composite effects of multiple cytokines are rarely tested • unknown cytokines may be involved in rejection • cytokine polymorphisms may explain variations • in-vitro effects may not reflect in-vivo effects • animal data may not translate into in clinical data • > nonreductionist research approach necessary Orosz CG. J Heart Lung Transplant 1996;15:1063 Baan et al. Transplant Int 1998;11:160 Bumgardner et al. Sem Liver Dis 1999;19:189
Recipient immune response Rejection Quiescence T-cell activating signals #1 T-cell receptor #2 CD28 #2a CD40L #3 IL2, IL15 etc phenome TCR metabolome CD3+ T-cell monocyte B-cell Allo Ag allo MHC Allo Ag self MHC proteome CD8+ CD4+ transcriptome allo APC self APC rejection CD4+Th1 CD8+ Cytotox CD4+/45RO+ genome Cardiac allograft tolerance CD4+/25+ CD8+ suppr CD8+28- suppr CD4+Th2 allograft rejection
differential lymphocyte homing Grant AJ et al. Lancet 2002;359:150
endomyocardial biopsy mild severe status quo monitoring future monitoring • invasive & complication-prone • late-stage cellular rejection diagnosis • insensitive for humoral rejection • significant variability • no insight into molecular mechanisms • resource-intense • highly sensitive for rejection • strong negative predictive value • positive test >need for further workup • non-invasive • easily repeatable on outpatient basis • low complication rate • decreased costs
systemic IL6 & HTx • 15 pts, < 3 mo posttx, at EMB time • IL6 ELISA, RHC, echo • IL2 & rej 2+ • IL6 & prognosis pg/ml IL6 300 200 250 MOF 150 200 150 100 stable 100 50 50 0 0 0 5 10 15 20 25 30 1 2 3 4 5 6 7 8 RAP Bx time Deng et al. Transplantation 1995;60:1118
HTx management malaise graft dysfunction immunosuppression under over infection cellul rej SIRS humor rej antibiotics bolus steroids cyclophosph reduced IS Deng et al. Transplantation 1998;65:1255
CARGO clinical study summary Overview CardiacAllograft Rejection Gene expression Observational study = “CARGO” 8 center, 4-year observational study initiated in 2001 (22% of US HTx). 629 patients, 4917 post-transplant encounters Hypothesis Gene expression profiling of peripheral blood mononuclear cells can discriminate ISHLT grade 0 rejection (quiescence) from moderate/severe (ISHLT grade ≥ 3A) rejection Design & Result Prospective, blinded validation study of 20 gene algorithm demonstrated ability to distinguish Grade 3A rejection from quiescence • Candidate geneselection • 285 Leukocyte microarray • Database / literature mining • 252 candidate genes I Discovery ~2 years (microarray) • Algorithm development • Real-time PCR • 20-gene algorithm to distinguish rejection from quiescence (AlloMap molecular testing) II Development ~1 year (PCR) III • Validation • Prospective, blinded, statistically-powered (n = 270) • Additional samples tested to further define performance (n > 1000) Clinical Validation ~1 year (Molecular Test) Deng/Eisen/Mehra et al. Am J Transplant 2006;6:150
Study Design Prospective Multi-center Non-blinded Randomized Non-inferiority Patients 2-5 years post-Tx ≥ 18 years old Stable outpatients Invasive Monitoring Attenuation through Gene Expression IMAGE Question How do theGEP-based study restrictions affect clinical implementation? • Hypothesis • To determine whether the monitoring of acute rejectionusing GEP is not inferior compared to the use of the EMB with respect to the event-free survival • Decrease in LV function, defined as LVEF change ≥ 25% compared with the baseline, or enrollment value, as measured by echocardiography • Development of clinically overt rejection (heart failure, hemodynamic compromise) • Death from any cause ClinicalTrials.gov identifier NCT00351559 Pham/Deng/Kfoury et al. J Heart Lung Transplant 2007;26:808
Gene Profiling Arm Study End Year 2 - 3 Year 4 - 5 Clinic x x x x x Echo x x x x x GEP/EMB x x x x x Enrollment Visit & Randomization Biopsy Arm ~2 year follow-up Invasive Monitoring Attenuation through Gene Expression IMAGE
Allomap implementation milestones • CARGO study start (2001) • CARGO study completion/CLIA approval (2005) • Allomap Medicare reimbursement (2006) • FDA approval IVDMIA (2008) • CARGOII Study (2009) • IMAGE Study (2010) 2005 2010 2000
regulatory transitions – CLIA>FDA • CLIA approval 2005 • FDA approval 2008 – safety & efficacy • Center for Devices & Radiological Health • In-vitro diagnostic multivariate index assay IVDMIA • FDA-director Daniel Schultz comment: “…Allomap is an example of how advancements in science and technology are leading to new medical care diagnostics…“
strategies in GEP test development Shahzad ,Sinha , Latif, Deng. Standardized operational procedures in clinical gene expression biomarker panel development. In: Scherer A (Ed).John Wiley & Sons 2009
dimensionality problem overview • The application of several high-throughput genomic and proteomic technologies generate high-dimensional data sets • The multimodality of high-dimensional expression data can confound both simple mechanistic interpretations of biology and the generation of complete or accurate gene signal transduction pathways or networks. • The mathematical and statistical properties of high-dimensional data spaces are often poorly understood or inadequately considered, particularly if the number of data points obtained for each specimen greatly exceed the number of specimens. • Data are rarely randomly distributed in high-dimensions and are highly correlated, often with spurious correlations. • The distances between a data point and its nearest and farthest neighbours can become equidistant in high dimensions, potentially compromising the accuracy of some distance-based analysis tools. • Owing to the ‘curse of dimensionality’ phenomenon and its negative impact on generalization performance, the large estimation error from complex statistical models can easily compromise the prediction advantage provided by their greater representation power. • Some machine learning methods address the ‘curse of dimensionality’ in high-dimensional data analysis through feature selection and dimensionality reduction, leading to better data visualization and improved classification. • It is important to ensure that the generalization capability of classifiers derived by supervised learning methods from high-dimensional data is independently validated Clarke R et al. Nat Rev Cancer 2008;8:37