Download
1 / 26
300 likes | 673 Vues
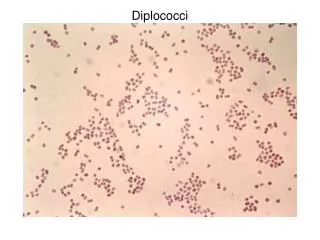
Molecular testing for Neisseria gonorrhoeae. J.Dave. Guidelines for molecular testing for Neisseria gonorrhoeae. Initiated and chaired by Dr Anne Eastaway, HPS

E N D
Guidelines for molecular testing for Neisseria gonorrhoeae Initiated and chaired by Dr Anne Eastaway, HPS Members/representatives: Drs Andy Winter and Kirsty Abu-Rajab (Sandyford), Bill Carman (Gartnavel) Alastair Leonard (Monklands), Lesley Wallace (HPS), Helen Palmer, Jayshree Dave and Hugh Young (SBSTIRL)
Guidelines for molecular testing for Neisseria gonorrhoeae: AIMS • To ensure that national surveillance for gonococcal infection is maintained • To determine the role of SNGRL in the introduction of routine molecular detection by nucleic acid amplification tests (NAATs) • To ensure as far as possible that the results from molecular tests are reliable
Drivers for detection of gonorrhoea by NAATs • Use of NAATs for chlamydia (SIGN) • Availability of dual CT/NG tests • eases burden on stretched GUM clinics • Small or no additional cost of NG testing • Independent of GC viability • Suitable for areas remote from laboratory • or any area where there is a delay in getting samples to the lab
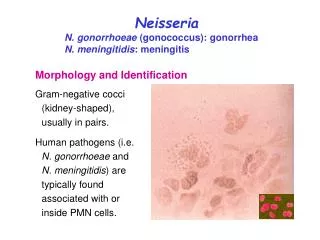
Performance of tests to detect gonococcal infection Diagnostic method Sensitivity Specificity Gram stain urogenital specimens Males -symptomatic 90-95% 95-100% Males - asymptomatic 50-70% 95-100% Females 50-70% 95-100% Culture Urogenital 80-95% 100% Rectal 50-60% 100% Pharyngeal 40-50% 100% NAATs (urogenital) 65-99% 91-100%
Recovery of 35 gonococcal isolates on transport swabs at room temperature (high inoculum) Mean inoculum 5.9 x 10 5 cfu/ml
Recovery of 35 gonococcal isolates on transport swabs at room temperature (low inoculum) Mean inoculum 5.9 x 10 3 cfu/ml
Currently available NAATs for combined detection of chlamydia and gonorrhoea • Cobas Amplicor CT/NG (Roche) • Roche Taqman real time PCR (only for CT) • GC under development • ProbTec ET SDA CT/NG (Becton Dickinson) • Aptima Combo 2 TMA (GenProbe) • Aptima GC (GenProbe) • Realtime CT/NG PCR – under evaluation (Abbott)
Aptima versus current diagnostic methods • Routine samples tested and reported as per laboratory SOPS • Chlamydia TaqMan with repeat testing of positives • Gonorrhoea culture – direct plating on modified NYC medium (10% lysed horse blood and LCAT) • Study samples tested by Aptima Combo2 and positives re-tested by mono-specific test • Study results not routinely reported to clinic • Study results reviewed weekly • Notify GUM if Aptima test Positive and routine test Negative • discordant result explained and treatment recommended
Gonorrhoea:1521 patient episodes Endocervical swabs *1 contact GC Correlation 99.8% (1518/1521)
Gonorrhoea: Sensitivity of Culture and Aptima in detecting infected women Prevalence: 0.6% (9/1521) or 0.5% (7/1521) Culture Sensitivity: 66.7% (6/9) or 85.7% (6/7) Aptima Sensitivity: 100% (9/9) or (7/7) Specificity 100% or 99.9% (1512/1514)
Gonorrhoea:1158 male episodes urethral culture versus urine Correlation 100% (1158/1158)
Gonorrhoea: 224 male episodes rectal culture versus Aptima Correlation 94.2% (211/224) all culture pos were Aptima pos *10 had additional evidence of gonococcal infection
Gonorrhoea: 242 male episodes throat culture versus Aptima Correlation 93.8% (226/241) all culture pos were Aptima pos *12 had supportive evidence of gonococcal infection
Gonorrhoea: Sensitivity of Culture and Aptima in detecting infected men * 4 no other evidence of gonorrhoea Prevalence: 3.5% (42/1205) or 3.2% (38/1205) Culture Sensitivity: 71.4% (30/42) or 78.9% (30/38) Aptima Sensitivity: 100% (42/42) or (38/38) Aptima Specificity: 100% (1163/1163) or 99.7% (1163/1167)
Gonorrhoea: Infected sites from 1205 male episodes Prevalence by Culture 2.5% (31/1205) Prevalence by Aptima 3.5% (42 /1205) or 3.2% (38/1205)
Conclusions on Aptima for GC • Aptima was more sensitive than culture in detecting cervical gonorrhoea (100% vs 66.7% or 85.7%) • Aptima was equivalent to culture in detecting urethral gonorrhoea in men (100% correlation) • Aptima was more sensitive than culture in detecting rectal gonorrhoea in men (100% versus 38% to 44%) • Aptima was more sensitive than culture in detecting throat gonorrhoea in men (100% versus 35% to 40%) • Overall Aptima detected 23% (7/31) to 35% (11/31) more gonococcal infections • A strategy is required to ensure antibiotic resistance surveillance when molecular diagnosis is used
Published data on specificity of NAATs for gonorrhoea 99.7% all sites 99.9%
Which NAAT ? Analytical Specificity • - results from testing a panel of relevant organisms • Test Cross Reacting organism • Cobas Amplicor N. flavescens, N. lactamica, N.sicca N.subflava N.cinerea • BD Probetec N. flavescens N. lactamica • N. subflava N cinerea • Aptima Combo 2 none to date • Aptima GC none to date • Some of these tests are more likely than others to generate false positives and decrease the Positive Predictive Value of a positive screening test
Guidelines for the introduction of NAATs • Test platform • May vary depending on local circumstances • Specimen • Male urine • Cervical or vulvo-vaginal swab (can be self-taken) • if urine from female is tested add comment “urine is sub-optimal for detecting gonorrhoea in women and will miss up to 1 in 4 infected women” • Supplemental testing is essential • Discussed with local lead clinician for GUM services • Local agreement between laboratory and GUM in terms of reporting initial test result • Non-GUM samples should always have a supplemental test before reporting • Patient with positive NAAT should be referred (and/or treated) to GUM for partner notification work
Supplemental NAAT testing • Scenario 1 • Diagnostic lab performs two separate NAATs each targeting a different region of DNA or RNA • Multiplex reaction • Two separate tests (ideally on a different platform) • Aliquot of original sample from all positives (or equivocals) sent to SBSTIRL for ST • Scenario 2 • Diagnostic lab performs a single NAAT • All positive and equivocal results sent to SBSTIRL for a supplemental NAAT targeting a different region of DNA or RNA
Culture & Introduction of NAATs • In addition to NAAT • Cultures should be taken in GUM patients as follows: • Symptomatic for gonorrhoea • Positive on Gram-stained smear • Known contact of gonorrhoea • Anyone treated on epidemiological grounds • Treatment failure • All return patients who are NAAT positive but not included above • All isolates sent to SBSTIRL • When NAAT is positive local laboratory identification of isolates can be restricted to oxidase positive GNDC • SNGRL will perform susceptibility testing and sequence typing • SNGRL will hold NAAT sample for up to 2 weeks prior to sequence typing to link with cultures
SNGRL and the introduction of NAATs • Advise on commercial systems, strengths & drawbacks • Provide supplemental testing during the period of introduction of NAATs until an acceptable level of concordance between laboratory results is established • Provide supplemental testing for labs that detect only one target • Perform sensitivity testing on all isolates received to advise on individual treatment and support national surveillance programme • Sequence type all strains either from NAAT or culture to support local contact tracing and National surveillance
* This pattern reflects either a false positive first test or a low level of nucleic acid
Acknowledgements • Hugh Young • Helen Palmer • GUM