Download
1 / 17
310 likes | 2.35k Vues
Neisseria N. gonorrhoeae (gonococcus): gonorrhea N. meningitidis : meningitis. Morphology and Identification. Gram-negative cocci (kidney-shaped), usually in pairs. Human pathogens (i.e. N. gonorrhoeae and N. meningitidis ) are typically found associated with or inside PMN cells.

E N D
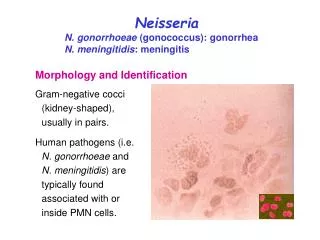
Neisseria N. gonorrhoeae (gonococcus): gonorrhea N. meningitidis: meningitis Morphology and Identification Gram-negative cocci (kidney-shaped), usually in pairs. Human pathogens (i.e. N. gonorrhoeae and N. meningitidis) are typically found associated with or inside PMN cells.
Morphology and Identification Both meningococci and gonococci are encapsulated: menigococci have a polysaccharide capsule; gonococci have a loose capsule-like structure. Grow best under aerobic conditions Produce oxidase (oxidase-positive). Meningococci and gonococci grow best in medium containing complex organic substances (e.g. blood, hemin, and animal proteins), and in an atmosphere containing 5% CO2. Meningococci and gonococci are rapidly killed by drying, sunlight, moist heat and many disinfectants. Poor survival at cooler temperature.
N. gonorrhoeae (Gonococcus) Form opaque and transparent variants; the opaque colonies are associated with the presence of Opa. Antigenic structure 3. Opa (protein II): an outer membrane protein functioning in attachment to host cells. 4. Rmp (protein III): stimulates Abs that block serum bactericidal activity. 5. Lipooligosaccharide (LOS): lacking long-antigenic side chains; endotoxic. 6. Other proteins. 1. Pili: enhancing attachment to host cells and resistance to phagocytosis; antigenically different among strains, and a single strain can make many antigenically distinct forms of pilin. 2. Por (protein I): forms porins and mediates resistance to serum killing. N. gonorrhoeae is capable of changing its surface antigens (pilin, Opa, and LOS) rapidly to avoid host defenses.
Pathogenesis and Pathology Gonococci attack mucous membrane of the genitourinary tract, eye, rectum, and throat, producing acute suppuration that lead to tissue invasion; this is followed by chronic inflammation and fibrosis.
Symptoms Male: urethritis with yellow, creamy pus and painful urination. The process may extend to the epididymis. As suppuration subsides in untreated infection, fibrosis occurs, sometimes leading to urethral strictures. Female: infection starts from the endocervix, then, urethra and vagina, giving rise to mucopurulent discharge. Uterine tubes may be involved, causing salpingitis, fibrosis, and obliteration of the tubes (20% may become infertile). 95% infected men and 50% infected women have acute symptoms. Asymptomatic carriage is more common in women than in men. Gonococcal bacteremia (1-3% of infected women and much lower percent of infected men) can lead to skin lesions, tenosynovitis and suppurative arthritis. Gonococcal ophthalmia neonatorum (purulent conjunctivitis in newborns); prevention: tetracycline, erythromycin or silver nitrate.
Immunity Treatments Repeated gonococcal infections are common, because protective immunity to reinfection does not develop due to the antigenic variation of gonococci. This makes development of effective vaccines difficult. Resistance to penicillin G (PPNG: penicillinase-producing N. gonorrhoeae) and tetracycline is common. Ceftriaxon can be used for gonococci. In gonococcal infections other than urethritis in men, cure should be established by follow-up, including cultures from the involved sites.
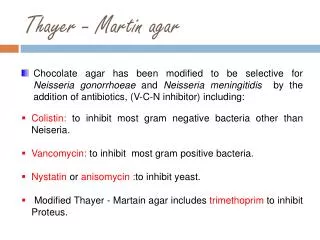
Laboratory Diagnosis Gram stain (gram-negative diplococci in PMNs): Sensitive (>90%) and specific (98%) for men with purulent urethritis. Less sensitive for asymptomatic men (<60%). Relatively insensitive for both symptomatic and asymptomatic women. * Negative results must be confirmed by culture. Culture: Avoid drying of specimen (genital or rectal) and low temperature. Inoculate both the selective media (e.g., modified Thayer-Martin) and non-selective media (e.g., chocolate blood agar; for strains that are sensitive to vancomycin).
Identification: N. gonorrhoeae is distinguished from other species by acid production from glucose but not from other sugars. Commercial genetic probes for direct detection of bacteria in clinical specimens.
【聯合新聞網】2004.10.29 自91年到93年,台北市接獲通報的梅毒及淋病患者都有顯著增加的趨勢,以淋病來說,91年的通報人數為257人、92年為469人,而今年9月為止就有375人,又以梅毒來說,91年通報數為667人,92年為637人,但今年不到10月就有690人感染,情況嚴重。 儘管通報人數有上升,但台北市性防所護理組主任莊苹卻表示,實際感染人數應該更多,因為許多人罹患性病都到小診所看病,而淋病與梅毒的通報必須檢驗確認才行,由於通報沒有獎金加上必須做檢驗,許多醫生為了省麻煩,只看了病人的性器官,就憑著症狀開藥,不做檢查也不通報。 不通報造成的後果就是,衛生單位無法追蹤性伴侶或配偶,也無法確認病患是否治療完成,這不但增加復發率,也增加交叉感染的危險性。
Epidemiology, Prevention, and Control Gonorrhea occurs only in humans. Gonorrhea is transmitted by sexual contact, often by women and men with asymptomatic infections. Chemoprophylaxis is of limited value. Areas with high incidence of PPNG: Asia, parts of Africa and some places in USA. Infection rate can be reduced by: 1. avoiding multiple sexual partners; 2. early diagnosis and treatment; 3. finding cases and contacts through education and screening of population at high risk.
N. meningitidis (Meningococcus) 【大紀元1月30日訊】安徽近期發生C群流腦疫情,自2004年12月20日~2005年1月28日,除了3名在南京死亡的安徽病人外,安徽還有5人死亡、7人隔離、49人治癒,61個「新型C群流行性腦膜炎」病例已涉及全省17個城市中的11個城市的22個縣(區)。 據安徽省衛生廳副廳長杜昌智說,自2004年12月下旬以來,在安徽蕪湖、滁州、安慶、巢湖、合肥等地的個別學校先後暴發流腦疫情,其他部分地區陸續出現散發病例。發病者以中小學生為主,占病例總數的77%,年齡多在13歲~18歲之間--已報告的在安徽死亡的5名死者,都是合肥、蕪湖、滁州等地的在校學生。 此次流腦疫情具有以下特點:一是流腦發病數比去年同期有所上升,由14例上升為61例;二是病例呈散發狀態,疫點涉及11個市的22個縣(區);三是引起流腦局部傳播流行的主要是C群腦膜炎雙球菌,這一群種是近年來新發現報告的菌群,冬春季節是此病的高發期。 C群流腦具有易傳播、隱性感染比例高、起病急、病程進展快、死亡率高等特點,臨床上常表現為暴發型、可在發病後24小時內死亡。C群流腦感染者以高熱為首發症狀、伴有頭痛、全身酸痛、咽痛、咳嗽等,部分病人出現皮膚瘀斑、瘀點,頸部強直、噴射性嘔吐等。
Antigenic structure 1. Capsular polysaccharide: more than 13 serogroups have been identified (serogroups A, B, C, X, Y, and W135 are most commonly isolated). 2. Pili 3. Outer membrane proteins: these are analogues to the Por and Opa proteins of gonococci. 4. Lipooligosaccharide (LOS): responsible for diffuse vascular damage in meningococcal infections. *Twenty serotypes have been identified based on the differences in outer membrane proteins and LOS.
Pathogenesis, Pathology, and Clinical Finding Meningococci are pathogenic only for humans under natural conditions. Both gonococci and meningococci are able to invade the epithelial cells. The capsule of meningococci protects the bacteria from phagocytic destruction. Nasopharynx is the portal of entry attach to epithelial cells with the aid of pili (may colonize without producing symptoms) reach the blood stream, producing bacteremia. Upper respiratory tract infection. Fulminant meningococcemia.
Fulminant meningococcemia High fever and hemmorrhagic rash. There may be disseminated intravascular coagulation and circulatory collapse. Meningitis is the most common complication of meningococcemia. Symptoms: begins suddenly, with intense headache, vomiting, and stiff neck, and progress to coma within a few hours. Meningococcemia can be prevented by specific bactericidal antibodies in serum.
Immunity Protective immunity is the group- or type-specific, complement dependent, bactericidal antibodies. Treatments Penicillin G is the drug of choice. Laboratory Diagnosis Specimen: blood and cerebrospinal fluid (CSF). >107 bacteria/ml of CSF are normally found in untreated patients. Gram stain: gram-negative diplococci in PMNs. Culture: alternative blood culture methods are required because additives in the blood culture broths can be toxic for this organism. Identification: acid formation with glucose and maltose, but not others.
Epidemiology, Prevention, and Control Meningococcal meningitis occurs in epidemic (in developing countries) and sporadic cases (in developed countries). Transmitted by respiratory droplets among people in close contact (family members; soldiers in military barracks; direct contact with the respiratory secretions of an infected person.) Reduction of personal contacts in a population with a high carrier rate is important for prevention. Riphampicin or minocycline can often eradicate the carrier state and serve as chemoprophylaxis. Vaccination of specific capsular polysaccharides of groups A, C, Y, and W-135 is used for protecting susceptible persons against infection.
Lipopolysaccharide (LPS) is also called endotoxin. LPS is composed of lipid A, core polysaccharide, and O-specific polysaccharide. Lipid Aanchors LPS in the lipid bilayer. It causes symptoms associated with endotoxin. O-specific polysaccharide can be used to identify certain species and strains. Back