Acute Inflammation
Acute Inflammation. Dr Margaret Burgoyne Department of Pathology Southern General Hospital. Acute Inflammation. Response of living tissue to damage Three main functions: Affected area is occupied by acute inflammatory exudate Infective agents destroyed

Acute Inflammation
E N D
Presentation Transcript
Acute Inflammation Dr Margaret Burgoyne Department of Pathology Southern General Hospital
Acute Inflammation • Response of living tissue to damage Three main functions: • Affected area is occupied by acute inflammatory exudate • Infective agents destroyed • Damaged tissues broken down and removed
Acute Inflammation-Causes • Microbial infection Viruses lead to cell death by intracellular multiplication Bacteria release specific exotoxins or have endotoxins associated with cell walls • Physical agents Physical trauma Ultraviolet or other ionising radiation Heat (Burns) Cold (frostbite)
Acute Inflammation -Causes • Irritant and corrosive chemicals Acids Alkali Oxidising agents Infective agents may release specific chemical irritants which lead directly to inflammation • Tissue necrosis Lack of oxygen or nutrients due to inadequate blood flow (infarction)
AcuteInflammation Clinical Features Cardinal signs described by Celsius: • Redness (rubor) due to dilatation of small blood vessels in damaged areas • Heat (calor) due to increased blood flow (hyperaemia) • Swelling (tumor) due to accumulation of fluid in extra vascular space (oedema) • Pain (dolor) Stretching/distortion of tissues due to oedema. Chemical mediators bradykinin, prostoglandins induce pain • Loss of function
The chief features are: 1. vascular dilatation 2.the formation of a fluid exudate 3. formation of a cellular exudate Acute Inflammation
Acute Inflammation Vascular congestion: dilated capillary Fluid exudate: Protein rich fluid moved from vessels to extravascular space
Acute Inflammation Normal polymorph Peripheral blood shows increased polymorphonuclear leucocytes
Acute Inflammation • Neutrophil Polymorphs: • Derived from precursors in bone marrow • Commonest white cell in blood • Increase in acute inflammation • Short life span in tissues • Motile • Chemotactic • Actively phagocytic
Acute Inflammation • Neutrophil polymorphs (cont): • Granules contain proteases • Kill bacteria by producing free radicles • Stimulate prostaglandin production
Acute Inflammation - Effects Beneficial effects Both the fluid and cellular exudates may have useful effects Fluid exudate: • Dilution of toxins • Entry of antibodies • Drug transport • Fibrin formation • Delivery of nutrient • Stimulation of immune response
Acute Inflammation - Effects Beneficial effects Cellular exudate (Neutrophils) • Adhesion to micro-organisms • Phagocytosis • Intracellular killing of micro-organisms – “respiratory burst” • Release of lysosomal products
Acute Inflammation - Effects Harmful effects • Digestion of normal tissues • Swelling • Inappropriate inflammatory response
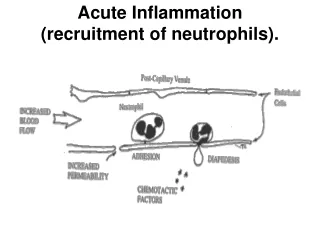
Acute Inflammation Early stages Oedema fluid, fibrin and neutrophil polymorphs accumulate in the extra- cellular spaces of damaged tissues. Acute inflammatory response involves 3 processes: • Change in blood vessel calibre and thus flow • Increased vascular permeability and formation of fluid exudate • Formation of cellular exudate by emigration of neutrophil polymorphs into the extracellular space
Acute InflammationEarly stages Acute inflammatory response (in brief) • Small blood vessels adjacent to the area of tissue damage initially become dilated with increased blood flow, then flow along them slows • Endothelial cells swell and partly retract so that they no longer form a complete intact internal lining • Vessels become “leaky” allowing passage of water, salts and small proteins from the plasma into the damaged area (exudation) • Circulating neutrophils initially adhere to the swollen endothelial cells (margination), then actively migrate through the vessel wall (emigration) into the area of tissue damage
Acute InflammationChanges in vessel calibre Triple response to injury (Lewis 1927) Momentary white line following injury due to arteriolar vasoconstriction, smooth muscle of arterioles contracting as a direct response to the injury Flush : dull red line due to capillary dilatation Flare : red irregular surrounding zone develops due to arteriolar dilatation Wheal: zone of oedema develops due to fluid accumulating in the extravascular space
Acute InflammationIncreased vascular permeability • Small blood vessels are lined by a single layer of endothelial cells forming a complete layer of uniform thickness around the vessel wall • Walls of small blood vessels acts as a microfilter allowing passage of water and solutes but blocking larger molecules and cells • O2, CO2 and some nutrients pass across the vessel wall by diffusion • Main transfer of fluid and solutes is by microfiltration
Acute InflammationIncreased vascular permeability Two mechansms for increased vascular permeability following tissue damage: • Toxins and physical agents may cause necrosis of vascular endothelial cells leading to abnormal leakage e.g. Burns • Chemical mediators of acute inflammation may cause retraction of endothelial cells leaving intercellular gaps e.g Histamine-immediate but transient response, Bradykinin, Complement C5a,C3a-delayed response
Acute Inflammation Dilated capillary Pavementing of neutrophils (margination) prior to emigration
AcuteInflammationChemotaxis of Neutrophils Movement of neutrophils from vessel lumen into damaged tissues is mediated by Chemotactic factors which diffuse from the area of tissue damage Main factors are: C5a, Leukotriene B4 and bacterial components • Margination (pavementing) • Emegration
Acute Inflammation • Endothelial cell: • Actively secretes many factors • Nitric oxide, prostacyclin • Induce vascular relaxation, prevent platelet aggregation • Endothelin, thromboxane A2, angiotensin II • Cause vascular constriction • Platelet Derived Growth Factor • Stimulates fibroblast mitogenesis
Acute Inflammation Phagocytosis 1. attachment to the opsonised bacterium 2. engulfment of the bacterium 3. discharge of the leucocyte granules into a phagosome (digestive vacuole) 4. killing and digestion of the bacterium within the phagocytic vacuole.
Acute Inflammation Polymorphs have ingested opsonised bacteria
Acute InflammationChemical mediators Chemical mediators released from cells cause vasodilatation, emigration of neutrophil, chemotaxis and increased vascular permeability Histamine: • causes vasodilatation and immediate transient phase of increased vascular permeability. • Stored in mast cells, basophils, eosinophils and platelets • Release is stimulated by C3a, C5a (complement) • Release is stimulated b lysosomal proteins released from neutrophils Lysosomal compounds • Released from neutrophils • Increase vascular permeability • Activate complement
Acute InflammationChemical mediators Prostaglandins • Long chain fatty acids derived from arachidonic acid • Potentiate increase in vascular permeability • Anti-inflammatory response to drugs such as aspirin or non-steroidal anti-inflammatory drugs is due to inhibition of enzymes involved in prostaglandin synthysis Leukotrienes • Synthesised from arachidonic acid especially in neutrophils • Vasoactive properties Serotonin (5 Hydroxytryptamine) • High Concentrations in mast cells • Vasoconstrictor
AcuteInflammationPlasma factors Plasma contains 4 enzymatic cascade systems: • Complement • Kinins • Coagulation factors • Fibrinolytic system These systems are inter-related and produce various inflammatory mediators
AcuteInflammationPlasma factors Complement system • Cascade system of enzymatic proteins • Activated during the acute inflammatory reaction by various methods • Enzyme release form dying cells in tissue necrosis • Antigen-Antibody complexes activate complement via Classical pathway • Endotoxins or other bacterial products activate complement via the Alternate pathway • Products of kinin, coagulation and fibrinolytic systems can activate complement
AcuteInflammationPlasma factors Products of complement activation with important actions in acute inflammation include: • C5a/C3a Chemotactic for neutrophils increases vascular permeability releases histamine from Mast cells • C567 Chemotactic for neutrophils • C56789 Cytolytic activity (membrane attack complex MAC) • C4b Opsonisation of bacteria • C2a Opsonisation of bacteria • C3b Opsonisation of bacteria
AcuteInflammationPlasma factors Kinin system • Peptides of 9-11 amino acids • Bradykinin most important vascular permeability factor • Activated by Coagulation factor XII (Hageman factor) • Bradykinin is a chemical mediator of pain Coagulation system • Conversion of soluble fibrinogen into fibrin • Fibrin is a major component ofthe acute inflammatory exudate • Coagulation factor XII once activated by contact with extracellular material e.g. basal lamina or proteolytic enzyes of bacteria can activate the coagulation, kinin and fibrinolytic systems Fibrinolytic system • Plasmin is responsible for lysis of fibrin into fibrin degradation products
Tissue Damage Serotonin Histamine C5a, C3a Leukotrienes Prostaglandins Nitric oxide C5a Leukotriene B4 Bacterial products Activation of vascular endothelim Dilatation of arterioles Activation of neutrophils Increased blood flow Increased leakiness of endothelium Neutrophils roll along endothelium Slowing of blood flow Increased adhesion Molecules on endothelium Plasma protein Into tissues Neutrophils adhere to endothelium Stasis of blood flow Neutrophil emegration • Immunoglobulins • Opsonisation • Activation of Complement • Inactivate organisms Fluid into tissues C5a Leukotriene B4 Fluid component of exudate Neutrophils migrate to site of Tissue damage (chemotaxis) • Complement • C3a, C5a • MAC • Opsonisation • Neutrophils • Phagocytose bacteria • Kill bacteria • Phagocytose tissue debris • Fibriongen • Fibrin framework • Immobilisation of organisms
Acute Inflammation Pus: dead and dying neutrophils Abscess: localised accumulation of pus Serous: clear fluid, low cell count Fibrinous exudate: high content of fibrin Seropurulent: fibrin +/- neutrophil leucocytes Purulent: massive accumulation of pnls
AcuteInflammationOutcome The sequelae of acute inflammation depend upon the type of tissue involved and the amount of tissue destruction, which depend in turn upon the nature of the injurious agent. The possible outcomes of acute inflammation are: • Resoultion • Suppuration • Organisation • Chronic inflammation
AcuteInflammationOutcome - Resolution Resolution - complete restoration of the tissues to normal May occur if: • Minimal cell death and tissue damage • Occurs in an organ or tissue with regenerative capacity • Raid destruction of causal agent • Rapid removal of fluid and debris by good vascular drainage
AcuteInflammationOutcome - Suppuration • Suppuration is the formation of pus • Usually due to infection with pyogenic bacteria • Once pus accumulates it is surrounded by a pyogenic membrane • Abscess • Bacteria within an abscess relatively inaccessible
AcuteInflammationOutcome - Organisation Organisation of tissues is their replacement by granulation tissue Usually results when: • Large amounts of fibrin are formed which cannot be removed by fibrinolysis • Large amounts of tissue necrosis occurs • Necrotic tissue is not easily digestible e.g. fibrous tissue • Exudate or debris cannot be removed or discharged During organisation new capillaries grow into the inflammatory exudate, macrophages migrate ad fibroblasts proliferate resulting in fibrosis.
Tissue damage or necrosis Acute Inflammation Marked neutrophilic response With tissue destruction Abcess formation Damage neutrolised Tissue damage minimal Damage neutrolised with tissue destruction Persisting damaging agent With tissue destruction Organisation through Phagocytosis and granulation tissue Organisation with continued inflammation Resolution Healing by organisation (Fibrosis) Chronic Inflammation