Oral Dexamethasone for Bronchiolitis: A randomized Trial
410 likes | 655 Vues
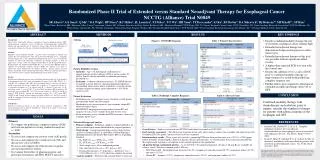
Oral Dexamethasone for Bronchiolitis: A randomized Trial. Journal club 20/2/14 Alansari K et al. Oral dexamethasone for bronchiolitis: a randomised trial. Pediatrics 2013 Oct;132(4):e810-6. Population. Qatar 2010- 2012 (bronchiolitis seasons) Infants ≤ 18 months

Oral Dexamethasone for Bronchiolitis: A randomized Trial
E N D
Presentation Transcript
Oral Dexamethasone for Bronchiolitis: A randomized Trial Journal club 20/2/14 Alansari K et al. Oral dexamethasone for bronchiolitis: a randomised trial. Pediatrics 2013 Oct;132(4):e810-6.
Population Qatar 2010- 2012 (bronchiolitis seasons) Infants ≤ 18 months “moderate to severe” bronchiolitis (Wang score ≥ 4) Bronchiolitis defined as viral URTI followed by wheezing or crackles on auscultation Hx of eczema or 1st degree relative with asthma Exclusions:- any previous wheeze, 02 sats ≤85%
Methods Assess on the acute ward CXR & NPA for every patient Randomise (concealed envelopes)
Intervention 1mg/kg dexamethasone for one day Then 0.6mg/kg per day for 4 days Or placebo
“Standard” Care Salbutamol Nebs at 0, 30, 60, 120 minutes then every 2 hours throughout admission Nebulsied Epinephrine 2.5- 5ml, if needed up to hourly
Primary Outcome Time from randomisation to ready for discharge as deemed fit by Dr on call (all patients get 6hrly review) - Decided does not need O2, ? Sats ≥ 94% - Feeding adequately - Minimal or absent wheezing, crackles or chest recessions
Secondary Outcomes Need for epinephrine Re-admission rates
Are the results valid? 1. Did the trial address a clearly focused issue? Yes
Are the results valid? 2. Was the assignment of patients to treatments randomised? Yes
Are the results valid? Were all the patients who entered the trial accounted for at its conclusion?
Is it worth continuing? 4. Were patients, health workers and study personel “blind” to the treatment? Yes
6. Aside from the intervention, were the groups treated equally? ?Yes
Will the results help locally?? 9. Can the results be applied in your context? No Not our standard care Not our definition of bronchiolitis Not same Dr levels/ review rates Primary outcome definition unclear
Bronchiolitis Research Many studies/ meta analyses Many definitions of bronchiolitis Many age ranges Many populations Many confounding factors Many outcomes (scores/ length of treatment/ length of stay
Definitions of Bronchiolitis UK “a seasonal viral illness characterised by fever, nasal discharge, dry, wheezy cough”. On examination there are fine inspiratory crackles and/ or high pitched expiratory wheeze Infants under 1 year of age
USA “a constellation of of clinical symptoms and signs including a viral upper respiratory prodrome followed by increased respiratory effort and wheezing in children less than 2 years”
Diagnosis Clinical ?NPA ?CXR
Schuh et al, 2007 (J Pediatr) 265 infants with simple bronchiolitis, all had CXR Only 2 CXRs not consistent with bronchiolitis (& neither case changed management) More likely to treat with abx after reviewing CXRs (although not indicated)
Aetiology • Viral upper -> Lower respiratory infection • Bronchiolar epithelial inflammation • Peribronchial infiltration of WBCs • Submucosal oedema • Airway narrowing through oedema and blockage with mucus (not smoothe muscle constriction)
Bronchodilators 8 trials, 468 infants No improvement in score in 43% treated with bronchodilators (57% in controls) Modest, short term effect in scores No change in other clinical measures (eg oxygenation) Authors conclude bronchodilators not recommended
Authors’ Conclusions Insufficient evidence to support use for inpatients. Possibly some benefit as outpatients Variety of definitions, outcomes and patient groups
Corticosteroids • Howard M et al, 2007 • 600 infants 2-12 months • Randomised to dex or placebo • No difference in scores, admission rates, clinical outcomes
? Benefit combined? • Hartling et al 2011 • Controversial meta-analysis • Accused of selection bias • Included children up to 2 yrs
Hypertonic saline • Zhang et al, 2013 • Hypertonic vs 0.9% saline • Infants <2 years • Conclude that length of stay reduced by hypertonic saline • But many confounding factors in studies analysed
SABRE: Hypertonic Saline in Acute Bronchiolitis: A Randomised Controlled Trial and Economic Evaluation