Restructure Medical Staff
Restructure Medical Staff Phase II Medical Staff History 1909 first Medical Staff was created to monitor quality in hospitals NO SIGNIFICANT CHANGE IN THIS STRUCTURE IN 100 YEARS Medicine now changing at rapid rate Pay-for-performance is HERE Current structure not agile Prelude

Restructure Medical Staff
E N D
Presentation Transcript
Restructure Medical Staff Phase II
Medical Staff History • 1909 first Medical Staff was created to monitor quality in hospitals • NO SIGNIFICANT CHANGE IN THIS STRUCTURE IN 100 YEARS • Medicine now changing at rapid rate • Pay-for-performance is HERE • Current structure not agile
Prelude • In 2000, at a Greeley Medical Staff Leadership Conference, we learned that most hospital have a two-year term for medical staff leaders • Looked at Medical Staff structures nation-wide and in our area • Rapid turnover of medical staff leaders and senior administration pointed to need for longer terms • We also researched with Health Care Advisory Board and had initial planning retreat in January with medical staff and Board. • We have had two subcommittee planning meetings in February and March of 2006 to develop OUR plan • We found the best structure was at Northwest Hospital and adopted it as our initial framework
Prelude Cont. • 2002 we implemented phase I of restructure • Started two-year terms for senior medical staff leadership, and created the Joint Operations Committee • We held off on phase II, due to financial concerns in early 2003 • We have had 6 months where we have had a retreat and planning subcommittee researching and revising our structure
Subcommittee Members • Ed Eissmann Tom Smith • Eli Saikaly Kevin Clay • Jeff Winningham Pat Ryan • Art Grossman Ival Salyer • Larry Nicolov Jim Brevig • Todd Gunderson Larry Schecter • Janice Halladay Bob McKnight • Ruth Felthous Judy Good • Yvonne Strader Sridar Chalaka
A Possible Solution • Unified Medical Staff Model • Goal is to combine and streamline the medical directors as well as the medical staff departments where appropriate and practical to meet the rapid changes in healthcare
Structure (Provisional) *MEC will review structure and adjust as needed *Specific specialties will elect their representative to work with section medical director. *Obligatory established contractual reporting requirements will be honored.
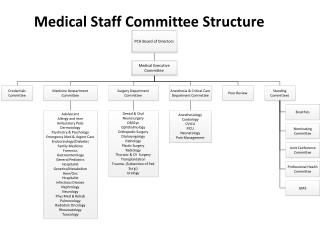
STRUCTURE DRAFT DRAFT
MEDICAL Behavioral Health FP IM Nephrology Neurology Rehab Sleep Lab Other as defined SURGICAL ENT GI GYN Hand Oto-Max Plastics Urology SPECIALTIES- DEFINED
SPECIALTIES- DEFINED • Out Patient Non-Hospital based • Allergy/Immunology • Behavioral Health (OP) • Dermatology • Endocrinology • Rheumatology • Others as defined
Structure Cont. • Ambulatory/Out Pt. Services Division • 300 MDs on Staff only practice in their offices • Create link to offices to assure that smooth transition of care from inpatient to outpatient. • There will continue to be specialty-specific recommendations for privileging by the Chairs/Directors of each section. (already doing this)
Does this do away with the Medical Staff Leadership? • Absolutely not ! • Medical Staff Leaders will still be delegated quality and credentialing by the Board of Directors • Medical Staff leadership will work closely with hospital administration and senior clinical leadership on operational issues • Medical Staff will actually have more input with the proposed new structure
Where Are We Now? • Senior Medical Staff Leadership, two-year terms • “Super” Medical Directors • Created Joint Operations Committee
Proposed Changes for Phase II • Division Chiefs • Medicine • Surgery • Family Services • Ambulatory /Out Pt. MDs
Division Chiefs • Two year terms, renewable (Conclusion of extension, 6 months prior to expiration of contract) • Nominated by Joint Operations (Board, Admin, Medical Staff) • Selection – may be nominated by division - and Interview Process • Final Candidate presented to Division • Approved by Division by simple majority • Initially ratified by MEC and Hospital Administration • Report to President of Medical Staff on medical staff concerns • Report to CMO for operational issues
Selection of Division Chiefs • Need to be an Active member of Medical Staff in good standing • Medical Staff and administrative experience preferred • Active 1/2 –time practice in community • If no internal candidate can be found and Medical Staff, Board, and Administration agree; then, an outside search would be started (e.g., Family Services)
Division Chiefs (continued) • Responsibilities: • Dyad model with Clinical Director for operations • Member of Credentials, MSQRC, Joint Operations and MEC • Responsible for QA, credentialing, and strategic planning in their division • Chair Quarterly QA for their division, and present issues to MSQRC • Implementation of policies for MEC • Have at least quarterly Division Meetings
Chief Responsibilities (continued) • Meetings with Section Directors at least quarterly or as needed • Time commitment 1/3 to 1/2 time • Compensation based on description and market equivalent • Annual ‘360 Review’
Section Medical Directors • Combines current medical directors with section chairs where appropriate • No additional medical directorships at section level • Responsible for QA, Credentialing, and planning in their section • Recommend clinical privilege criteria to Division Chief • Two-year term (may be renewed similarly to Division Chiefs) • Attend division QA Meetings, and other appropriate meeting as needed • Dyad Model with Clinical Director/Manager for operations
Section Medical Directors Cont. • Nominated by MEC and/or section, and Hospital Administration • Selection and Interview process • Candidate presented to Section • Confirmed by simple majority of section vote • Ratified by MEC and Hospital Administration • Work closely with clinical administration on issues in their area • Compensation, hourly for medical staff issues plus medical director fees • Report to Division Chief • Annual evaluation by section • Not all sections will have their own medical director
Medicine Hospitalists Medical Specialties ED Radiology Oncology Services Surgery General Surgery Orthopedics Surgical Sub-Specialties Pathology Anesthesiology Division Structure
Family Services OB/Gyn Peds (In-pt) FP-OB Midwives Specialty Services from Children's Community Out-pt FPs Out-pt IM Out-pt Peds Out-pt Specialty Division Structure
New MEC • Membership • Four, elected Senior Medical Staff - voting • Four Division Chiefs - voting • Hospital Senior Administration • Hospital Board Representation • Credentials Chair - voting • MSQRC Chair - voting
How Do We Compare? • Recently, several Medical Staff leaders, Board and Administration attended a governance seminar • Our proposed new structure was reviewed by Linda Haddad, a leading consultant on Medical Staff Issues • She was very complimentary of our structure • We are actually ahead of the curve
Election of Future* Division Chiefs • Nominated by MEC, or division • Interview and selection process • Candidate presented to Division • Voted on by Division (see above) • Need to meet qualifications of Division Chief as outlined previously
Question? • How do we elect Division Chiefs • Nominated by Nominating committee or division, Approved by simple majority • Ratified by MEC and Hospital Administration • They will have two year contracts, with annual review • They will have dual reporting to President Medical Staff and CMO • They will work closely with clinical directors • Compensated by Hospital • Officers will be elected as usual as well as members of MSQRC and Credentials
Potential Cost Off-sets • Potential reduction in current medical director positions/hours • Potential reduction in hours paid for meeting attendance by medical staff • Stipend from Medical Staff for medical staff issues
Benefits for Hospital • Aligns Medical Staff leadership to effectively meet challenges in our rapidly changing market • Establishes a leadership pool of MDs that will be responsible to implement operational issues with the medical staff • Has the potential to return much more on the investment, due to easier implementation of operational issues • Creates the framework for true partnership with the medical staff
Benefits for the Hospital • Potential savings based on Chiefs becoming champions: • Decreased Average Length Of Stay • Decreased resource utilization through standardization • Improved compliance with Core Measures and Pay-for-Performance measures • Improved Regulatory Readiness • Potential performance incentive programs
Next Steps Change Bylaws (Bylaws Committee working on new changes) • Vote on by Medical Staff (early Fall) • If approved by Medical Staff, set up the interview process for Division Chiefs and Section Medical Directors • Target Implementation around January 2007