Thoracic Outlet Syndrome
440 likes | 1.49k Vues
Thoracic Outlet Syndrome. Elana Deacon. Definition . Thoracic outlet syndrome (TOS) is a syndrome involving compression at the superior thoracic outlet where excess pressure is placed on a neurovascular bundle passing between the anterior scalene and middle scalene muscles.

Thoracic Outlet Syndrome
E N D
Presentation Transcript
Thoracic Outlet Syndrome Elana Deacon
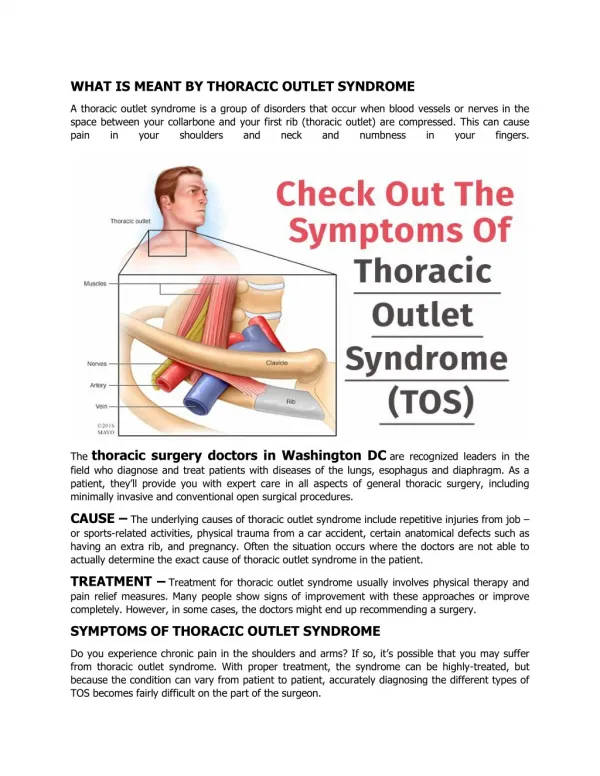
Definition • Thoracic outlet syndrome (TOS) is a syndrome involving compression at the superior thoracic outlet where excess pressure is placed on a neurovascular bundle passing between the anterior scalene and middle scalene muscles. • It can affect one or more of the brachial plexus nerves, the subclavian artery, and - rarely - the vein, which does not normally pass through the scalene hiatus.
Definition • TOS may occur due to a positional cause - for example, by abnormal compression from the clavicle and shoulder girdle on arm movement. • There are also several static forms, caused by abnormalities, enlargement, or spasm of the various muscles surrounding the arteries, veins, and/or brachial plexus, a fixation of a first rib, or a cervical rib. • Common orthopaedic tests used are the Adson's test, the Costoclavicular Manoeuvre, and the "Hands-Up" test. Careful examination and X-ray are required to differentially diagnose between the positional and static aetiologies, first rib fixations, scalene muscle spasm, and a cervical rib or fibrous band
Pathophysiology Neurovascular structures run from the thorax to the upper extremities through the thoracic outlet. Four areas are seen where these neurovascular bundles undergo compression: • Superior Thoracic Outlet • Scalene Triangle • Costo-clavicular Area • Pathway of the Coracoid Pectoralis
Pathophysiology • TOS involves compression, injury, or irritation to the neurovascular structures at the root of the neck or upper thoracic region, bounded by the anterior and middle scalenes; between the clavicle and first rib or beneath the pectoralis minor muscle. • The syndrome of compression at this site could be primarily neurologic, involving the brachial plexus, most often the lower trunk or medial cord • It could involve compression of the subclavian artery and/or vein. Thrombosis, embolus, or aneurysm of these vessels is a less likely possibility. • In addition, imaging with diagnostic ultrasound has been able to identify deformation of the pectoralis minor in TOS that may be related to the pathophysiology, due to excessive tightness or shortening of the muscle that impinges on the neurovascular bundle.
Pathophysiology • By structures affected & symptomatology • There are three main types of TOS, named according to the cause of the symptoms. • The compression can occur: • In three anatomical structures: arteries, veins and nerves • Can be isolated: two or three of the structures are compressed to greater or lesser degrees. • Neurogenic TOS: Disorders produced by compression of components of the brachial plexus nerves. Accounts for 95% of all cases of TOS. • Arterial TOS: Due to compression of the subclavian artery. • Venous TOS: Due to compression of the subclavian vein.
Pathophysiology • By event • Trauma • Sudden (Clavicle fracture caused by a car accident) • Repetitive (Legal secretary who works with his/her hands, wrists, and arms at a fast paced desk station with non-ergonomic posture for many years). • Occupations involving lots of lifting of the arms and repetitive use of the wrists and arms. E.g. swimmers, volleyball players, weightlifters, rock climbers, and electricians
Pathophysiology • By structure causing constriction • Classify TOS by the location of the obstruction: • Scalenusanticus syndrome = Compression on brachial plexus and/or subclavian artery caused by muscle growth Diagnosed by using Adson's sign with patient's head turned outward. • Cervical rib syndrome = Compression on brachial plexus and/or subclavian artery caused by bone growth Diagnosed by using Adson's sign with patient's head turned inward.
Pathophysiology • Costo-clavicular syndrome = Narrowing between the clavicle and the first rib. Diagnosed with the costo-clavicular manoeuvre. • Some people are born with an extra incomplete and very small rib above their first rib, which protrudes out into the superior thoracic outlet space. • Causes fibrous changes around the brachial plexus nerves, inducing compression and causing the symptoms and signs of TOS. • This is called a "cervical rib" because of its attachment to C-7 and its surgical removal is almost always recommended. The symptoms of TOS can first appear in the early teen years as a child is becoming more athletic.
Causes • Trauma i.e. whiplash from a motor vehicle accident, • Repetitive activities i.e. job duties • Poor posture i.e. forward head, and forward shoulders • Anatomical abnormalities i.e. extra rib or abnormal positioning • Entrapment at the costo-clavicular space (space between the first rib and collarbone) i.e. back pack or purse over shoulder, carrying heavy objects. • A Pancoast tumor(a rare form of lung cancer in the apex of the lung) may be the cause.
Risk Factors • Abnormal Scalene Triangle • Cervical Rib • Fibro-muscular Band • Elongated Transverse Process of C7 • Poor Posture • Age • Neck Spasms • Obesity • Pregnancy
Sign and Symptoms • Depends on specific structures that are being pinched • Structures that may be impinged: Brachial plexus Subclavial arteries • Neurological, vascular or both • Loss of sterognosis and fine co-ordination • Clumsiness of the hands • Swollen hands / hands feel heavy and lame • Fingers feel numb / cramps in fingers • Vascular symptoms worsen with elevation of the shoulders and if heavy object is carried, i.e. jacket
Signs and Symptoms • Neurological Symptoms: • Pain (Neuralgia / Nerve Root) • Abnormal sensation • Weakness • Vascular Symptoms: • Pain (Ischaemic) • Weakness • Claudication
Signs and Symptoms • Aggravated by abduction of arm • Onset: Usually spontaneous Followed after trauma of arm or neck • Neurological signs seen with the 3 min stress test • Vascular signs seen with abduction, extension and lateral rotation during palpation of the radial pulse No changes – rotation of head or deep breathing added Positive test shows signs of: Pain Reduced pulse Pallor of hands
Consequences • Pain that can be sharp, burning, or aching. • It can involve only part of the hand (as in the 4th and 5th finger only), all of the hand, or the inner aspect of the forearm and upper arm. • Pain in the side of the neck, the pectoral area below the clavicle, the axillary area, and the upper back (i.e. the trapezius and rhomboid area). • Decoloration of the hands, one hand colder than the other hand, weakness of the hand and arm muscles, and tingling are commonly present. • TOS is often the underlying cause of refractory upper limb conditions like frozen shoulder and carpal tunnel syndrome that frequently defy standard treatment protocols.
Consequences • Related to Cerebrovascular arterial insufficiency when affecting the subclavian artery. • Affect the vertebral artery - Producing transient blindness, and embolic cerebral infarction. • A painful, swollen and blue arm, particularly when occurring after strenuous physical activity, could be a sign of a venous compression or subclavian vein thrombosis.
Medical Management • Most patients respond to conservative measures: • Medications • Rest • Relaxation exercises • Chiropractic or physical therapy • Stretching of m. Scaleni and M. Trapezius • Posture correction • Handling of fear and ignorance • Exercises of strengthening of pectoral girdle • Mobilisation of 1st rib, cervical as well as upper and mid-thoracic • Trigger points in m. Scaleni and m. Trapezius • Only a minority of patients with signs and symptoms of TOS ultimately proceed to surgery. Resection of 1st rib or clavicle
Evidence-Based Article Physical Medicine and Rehabilitation for Thoracic Outlet Syndrome • Frequency • United States • The inability to make a definitive and accurate diagnosis makes determination of the exact prevalence of this condition impossible. The prevalence of nonspecific thoracic outlet syndrome (TOS) has been reported as high as 23% of soft-tissue injuries of the cervical spine. • Mortality/Morbidity • No known mortality is associated directly with thoracic outlet syndrome (TOS). Morbidity often encompasses debilitating functional loss of the involved upper extremity, loss of livelihood or occupation, especially if the work involves overhead activity (e.g. hairdressing, carpentry, painting). • Sex • Females are diagnosed more commonly with thoracic outlet syndrome than males, with some reports of a 9:1 female-to-male ratio. • . Age • Age of onset is from the second to the eighth decade, with a peak occurring in the fourth decade
Evidence-Based Article • Progressive postural decompensation with neurovascular compression. A: Normal resting posture. B: Shoulder protraction beginning; the sternomastoid muscles are shortening, drawing the head anteriorly and inferiorly. C: Advanced deformity with adaptive shortening of scalene and pectoralis minor muscles. Also note narrowed costo-clavicular space (ribs 1-5 have been relatively elevated). Neurovascular compression is evident at all 3 sites.
References • Lee J., Laker S., Fredericson M.I. 2010. Thoracic outlet syndrome. Physical Medicine & Rehabilitation. 2:64-70. (http://emedicine.medscape.com/article/316715-overview). retrieved on 19 August 2012. • Laulan, J., Fouquet, B., Rodaix, C., Jauffret, P., Roquelaure, Y., Descatha, A. 2011. Thoracic outlet syndrome: definition, aetiological factors, diagnosis, management and occupational impact. 21(3):366-73. (http://www.ncbi.nlm.nih.gov/pubmed/21193950). Retrieved on 19 August 2012. • Neuromusculo-skeletal Rehabilitation Dictate. Thoracic Outlet Syndrome. Pg. 208.