
osteoporosis
osteoporosis. Dr. Khosro K. Kalantari Associate professor Department of physiotherapy Shahid Beheshti University of Medical Sciences. OSTEOPOROSIS: “The Silent Disease”. “Osteo” is Latin for “bone” “Porosis” means “porous or full of holes”

osteoporosis
E N D
Presentation Transcript
osteoporosis Dr. Khosro K. Kalantari Associate professor Department of physiotherapy Shahid Beheshti University of Medical Sciences
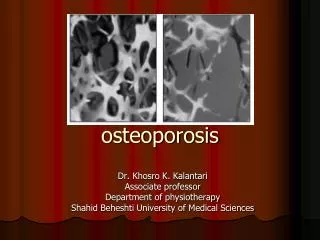
OSTEOPOROSIS: “The Silent Disease” “Osteo” is Latin for “bone” “Porosis” means “porous or full of holes” “Osteoporosis” means “bones that are full of holes” Osteoporosis can develop without symptoms You may not know you have the disease until a bone fractures
Epidemiology world • Internationally, over 50% of women and 30-45% of men over age 50 have osteopenia/osteoporosis • White woman over age 50: 50 % lifetime risk of osteoporotic fracture, 25% risk vertebral fracture, 15% risk of hip fracture • Man over age 60 has 25% risk osteoporotic fracture Iran • 47% of women and 44% of men above 50 are osteopenic/osteoporosis in Iran. • Average BMD of healthy Iranian people is 3.9% more than Japanese and 4.6% lower than Americans. • One in 4 Iranian women above 50 has osteoporosis. • Some studies reported that half of Iranian women above 45 and 90% of women above 75 have osteoporosis
TYPES OF BONE • 1- Cortical: • is hard, compact, dense bone • Runs the length of the long bones, forming a hollow cylinder • 2- Trabecular: • Has a honeycomb structure, is spongy, porous and flexible bone. • Occurs in the heads of the long bones • Also makes up most of the bone in the vertebrae
HEALTHY BONE Bone is living tissue, which is constantly being broken down and rebuilt, a process called remodeling Bone is renewed like skin, hair and nails
OSTEOPOROTIC BONE The loss of living bone tissue makes bones fragile and more likely to fracture Note: arrow points to micro - fracture
BONE REMODELING • Proceeds in cycles – first resorption then bone formation • The calcium content of bone turns over with a half-life of 1-5 years • Bone turn over take places in 3 phases.
BONE “REMODELING” Osteoclasts: Resorption-removes old bone Osteoblasts: Formation-replaces old bone with new bone
PHASE 1 • Signal from osteoblasts • Stimulation of osteoblastic precursor cells to become osteoclasts • Process takes 10 days
OSTEOCLASTS-PHASE 2 Cells called osteoclasts seek out old bone or damaged bone tissue and destroy it. Macrophages clean up leaving small spaces (resorption).
OSTEOBLASTS – PHASE 3 Cells called osteoblasts use minerals like calcium, phosphorus, and vitamin D to fill in the spaces with new bone (formation). Takes 3 months
BUILD YOUR BONE BANK You build bone until about age 30 Steps to building healthy bones include: Calcium & vitamin D Limit Caffeine & Alcohol Exercise Don’t Smoke
BONE BANK DEPOSITS - From birth through adolescence, new bone is built faster than old bone is removed - In mid-life, depending on lifestyle and other factors, bone removal can achieve a balance with bone formation - After menopause, bone removal may accelerate due to a decrease in estrogen
BONE LOSS & AGING The first 5-15 years after menopause a woman can lose approximately 25 - 30 % of trabecular bone & approximately 10 – 15 % of cortical bone Bone loss often occurs without symptoms or warning signs
CHANGES IN BONE MASS After menopause, bone removal accelerates due to a decrease in estrogen
EARLY WARNING SIGNS History of broken bones as an adult Unexplained back pain – subsides after a couple of weeks Loss of more than an inch in height Posture has become stooped
Vitamin D • Parathyroid Hormone • Calcitonin • Estrogen • Androgen
VITAMIN D • Osteoblast have receptors for vit D • Increases activity of both osteoblasts and osteoclasts • Increases remodeling • Increases mineralization through increased intestinal calcium absorption • Feedback action of vit D represses gene for PTH synthesis
PARATHYROID HORMONE • Accelerates removal of calcium from bone to increase Ca levels in blood • PTH receptors present on both osteoblasts and osteoclasts • Osteoblasts respond to PTH by Inhibition of collagen synthesis • Chronic stimulation of the PTH causes hypercalcemia and leads to resorptive effects of PTH on bone
CALCITONIN • C cells of thyroid gland secrete calcitonin • Rise in plasma calcium is major stimulus of calcitonin secretion • Plasma concentration is 10-20 pg/ml and half life is 5 min • Osteoclasts are target cells for calcitonin • Major effect of clacitonin is rapid fall of plasma calcium concentration caused by inhibition of bone resorption
OTHER HORMONES • Estrogens - Increase bone remodeling • Androgens - Increase bone formation • Growth hormone • Increases bone remodeling • Glucocorticoids • Inhibit bone formation • Thyroid hormones • Increase bone formation
RISK FACTORS
RISK FACTORS - CAN’T CONTROL • Gender: • - Females are usually diagnosed with osteoporosis at four to five times the rate of males. • - Bone mass in males is approximately 15-20% higher than females. • Women are smaller and start out with less bone. • they also lose bone tissue more rapidly as they age. • while women commonly lose 30-50% of their bone mass over lifetime, men lose only 20-33%.
Small Boned & Thin: - Women with small bones and those who are thin are more liable to have osteoporosis. - this results in smaller bones with a lower bone density
RISK FACTORS - CAN’T CONTROL • Race/Ethnicity: • - Women, especially Caucasian and Asian women (white) are at greater risk. • African American women have a higher peak bone mass (10%) than Caucasian women.
RISK FACTORS - CAN’T CONTROL • Heredity: • your family history may put you genetically at risk. • Research in Europe reported in 2003 that variations of a gene on chromosome 20 might make some postmenopausal women more likely to have osteoporosis. • It is possible that this could be a result of family members sharing the same environment, exercise, and nutritional habits
RISK FACTORS – CAN CONTROL • Menopause or several months without periods: - bone loss begins to exceed bone formation, due to a decrease of estrogen. - Up to 5% loss/year during first 5 years after menopause. - in the 5 to 7 years post menopausal women lose about 20% of their bone mass.
RISK FACTORS - CAN’T CONTROL • Age: • In your 40’s you start to lose bone faster than you build new bone. • The accumulated loss of bone puts an older person at higher risk.
RISK FACTORS – CAN CONTROL • Calcium Rich Diet: • milk, cheese, yogurt • Weight Bearing Exercise: • walk, bike, run • Vitamin D: • sunshine, multivitamin, fortified food
RISK FACTORS – CAN CONTROL Caffeine: No more than 2-3 cups of caffeine beverages per day Cola, coffee and chocolate all contain caffeine
RISK FACTORS – CAN CONTROL Alcohol: consuming alcoholic drink is associated with risk of low bone mass Eating Disorders: Anorexia nervosa or bulimia can lead to malnutrition and bone loss
RISK FACTORS – CAN CONTROL Smoking: causes lower bone density Immobility: extreme lack of exercise can lead to bone loss
OTHER RISK FACTORS Steroids - cause increased bone breakdown and decreased bone replacement Prolonged hyperparathyroidism – can cause increased risk of bone loss Hypothyroidism – acts on bone cells to increase resorption
OTHER RISK FACTORS Diuretics – some types of diuretics may increase excretion of calcium in the urine Kidney failure – affects the metabolism of calcium, phosphorous and vitamin D Chronic hepatitis – chronic liver disease may cause bone loss in several different ways Intestinal disease – some can affect the absorption of vitamin D & calcium
DRUGS-MAY CAUSE BONE LOSS Cortisone (immune-suppressor) Seizure drugs Cyclosporine (immune-suppressor) Methotrexate (antimetabolite, cancer &autoimmune dis) Isoniazid (antituberculosis, antidepressant ) Lithium (manic episodes of bipolar disorder) Heparin (anticoagulant)
TYPES OF OSTEOPOROSIS • Postmenopausal osteoporosis (type I) • Caused by lack of estrogen • Causes PTH to overstimulateosteoclasts • Excessive loss of trabecular bone • Age-associated osteoporosis (type II) • Bone loss due to increased bone turnover • Malabsorption • Mineral and vitamin deficiency • Secondary osteoporosis (Type III)
WHO NEEDS TESTING? • All women 65 years and older • Postmenopausal women <65 years of age with: • One or more risk factors • History of fracture
Who Should Be Considered for Prevention or Treatment? • Postmenopausal women with T-score below –2.0 with no risk factors • Postmenopausal women with T-score below –1.5 with one or more risk factors
SCREENING TESTS Portable scanners: SXA - (Single Energy X-ray Absorptiometry), measures wrist or heel pDXA - (Peripheral Dual Energy X-ray), measures wrist or heel
SCREENING TESTS RA - (Radiographic Absorptiometry), x-ray of hand that is compared to a small metal wedge QCT - (Quantitative Computed Tomography), measures the spine Ultrasound - sound waves to measure the heel, shin, and kneecap


















