Download
1 / 1
10 likes | 124 Vues
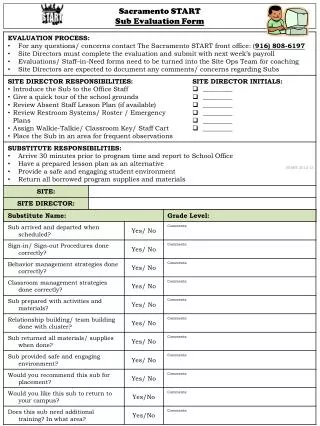
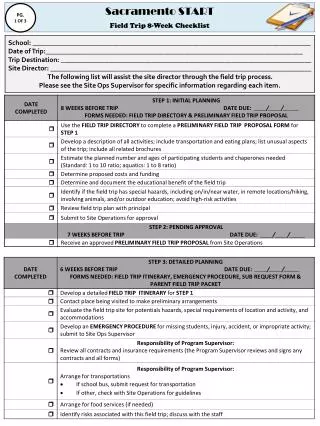
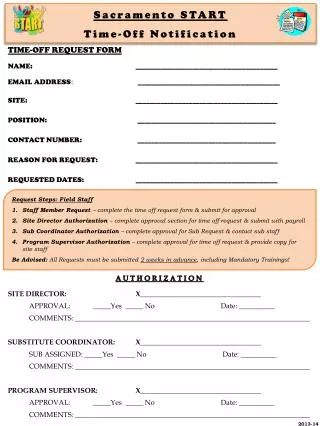
This Time-Off Request Form is essential for Sacramento staff to formally request time off. Employees must complete all sections, including their name, email, site, position, contact number, reason for the request, and the requested dates. It's important to follow the request steps, which include submission to the Site Director for authorization and coordination with the Substitute Coordinator and Program Supervisor. Please ensure all requests are submitted at least two weeks in advance, including any mandatory training.

E N D
Sacramento STARTTime-Off Notification TIME-OFF REQUEST FORM NAME: ________________________________________ EMAIL ADDRESS:________________________________________ SITE: ________________________________________ POSITION: _______________________________________ CONTACT NUMBER: _______________________________________ REASON FOR REQUEST: ________________________________________ REQUESTED DATES: ________________________________________ Request Steps: Field Staff Staff Member Request – complete the time off request form & submit for approval Site Director Authorization – complete approval section for time off request & submit with payroll Sub Coordinator Authorization – complete approval for Sub Request & contact sub staff Program Supervisor Authorization – complete approval for time off request & provide copy for site staff Be Advised: All Requests must be submitted 2 weeks in advance, including Mandatory Trainings! AUTHORIZATION SITE DIRECTOR: X__________________________________ APPROVAL: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ SUBSTITUTE COORDINATOR: X__________________________________ SUB ASSIGNED: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ PROGRAM SUPERVISOR: X__________________________________ APPROVAL: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ 2013-14