Download
1 / 63
640 likes | 774 Vues
Disturbances of external ventilation. Prof. J. Hanáček, M.D., Ph.D. Respiration - movement of oxygen from atmosphere to the cells and return of carbon dioxide from cells to the environment. External respiration : movement of air from atmosphere to

E N D
Disturbances of external ventilation Prof. J. Hanáček, M.D., Ph.D.
Respiration- movement of oxygen from atmosphere to the cellsand return of carbon dioxide fromcells to the environment External respiration :movement of air from atmosphere to the lung and from the lung to atmosphere 1. lung ventilation 2. distribution of air in lung 3. diffusion of gases across the A– c membrane 4. perfusion of lung by blood 5. distribution of blood in lung 6. ventilation - perfusion ratio
Internal respiration- refers to the intracellular chemical reactions in which oxygen and substrates are used andcarbon dioxide and other metabolitesare produced The lecture isdevoted to external respiration–toits disturbances Any disease of respiratory system (RS), diseases of other body systems and organs of men, may lead to changes ofcomponents of external respiration Lung ventilation (LV) is able to compensate partially ortotally the disturbancesof air distribution, diffusion of gases and perfusion blood in lungs !! Renew your knowledge on anatomy, histology and physiology of respiratory system
VD VT VL VA VD Vtot VA
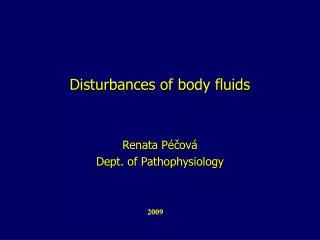
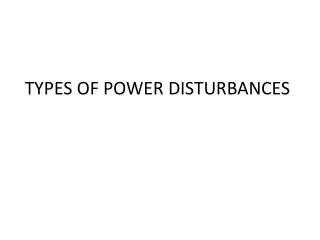
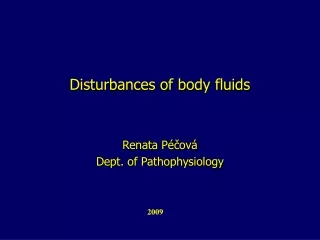
Lung ventilation and mechanisms involved in its disturbances LV - movement of air in and out of the lungs The main role of LV is to provide required O2 and CO2 concentration in the alveoli Alveolar unit • it is outlined as spherical structure containing gas(alveolar volume = VA) • connected to the outside airby a tube (dead space volume = VD) -gas exchange between the blood and air takes place in the acinus, mainly in alveolar space, not in dead space
Lung volume (VL) : VA + VD = VL Lung dead space ( VD) : • anatomical dead space (VD,an) • alveolar dead space (VD,A) • functional dead space (VDf): volume of that part of the • respiratory tract and alveoli which is not involved in the • exchange of gases between the blood and inhaled air Total ventilation(respiratory output, Vtot.): the air volumeflowing to or from the lung per unit of time (respiratory rate X tidal volume) Alveolar ventilation(VA): the portion of Vtot which flows into the alveolar space Dead space ventilation(VD): the portion of Vtot which doesnot contribute to alveolar gas replacement
Note ! • Intensity of alveolar ventilationis reflected byPO2 and PCO2 • in alveolar space b)The intensity of alveolar wash out is determined by the ratio of VA/VA A low value indicates low intensity of alveolar gas replacementalveoli areunderventilated c)The intensity of alveolar wash out is determined also by t he ratio of VD to VA A high value indicates bad alveolar ventilationalveoli are underventilated
Ad b)Changes in total alveolar volume may be due to: -increase (growth of the lung, exercise?) ordecrease number of alveolar units (pneumonia, edema, senescence, lobectomy, pneumonectomy) - increase (emphysema) or decrease of the size ofthe alveolar units (pneumonia, edema,pulmonary fibrosis)
With respect to alveolar ventilation, the following terminology is used • normoventilation-VA corresponds (is matched), to the metabolic • rateof tissue ofthe whole body normocapnia • ofthe arterial blood 2. hypoventilation- VA is low in proportion to the metabolic ratehypercapniaof the a. blood 3. hyperventilation- VA is high in proportion to the metabolic rate hypocapnia of the a. blood
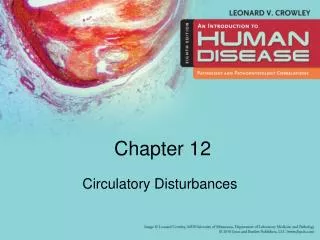
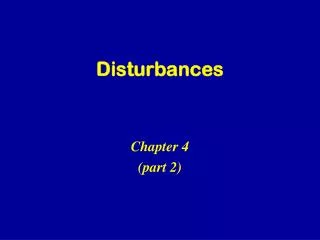
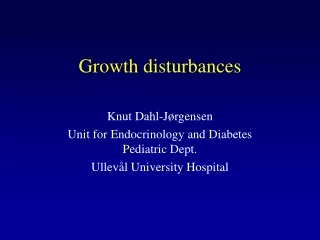
Alveolar hypoventilation is very important and very frequent cosequence of respiratory diseases What basic machanisms are involved in development of alveolar hypoventilation ? • VA normal, VAis decreased(e.g.respiratory center inhibition, • airway obstruction…) b) VAis increased, VA is normal (e.g. emphysema pulmonum ) c) VA and VA are normal, butVD is increased(e.g. ventilated but not perfused alveoli) ! Try to deduce from presented scheme the pathological events which can be involved in onset of alveolar hyperventilation!
H Y P O V E N T I L A T I O N Physiologic VA VA VD VE VI H Y P E R V E N T I L A T I O N VA VA VA VD
Pathological processes involved in disturbances of alveolar ventilation Alveolar hypoventilation I. Extrapulmonary causes A. Central nervous system dysfunction 1. Drug induced inhibition of respiratory centres 2. Infection processes (e.g. bulbar polio etc.) 3. Trauma 4. Idiopathic depression of the respiratory centre (Ondines curse) Ondine
B. Peripheral nervous system • Guillain - Barré syndrome – Acute inflammatory demyelinating • polyradiculoneuropathy 2. Different forms of polyneuritis 3. Poliomyelitis 4. Trauma (spinal cord, phrenic nervs damage etc.) C. Primary or secondary myopathy 1. Myasthenia gravis 2. Adverse reactions to curare 3. Other forms of myopathy (myositis, myalgia, respiratory muscles fatique)
D. Metabolic causes 1. Metabolic alkalosis 2. Hypothyroidism E. Chest wall 1. Kyphoscoliosis 2. Obesity 3. Trauma, surgery
II. Pulmonary (airway) causes A. Obstruction of central airways– e.g. obstructive sleep apnoea sy B. Obstruction of peripheral airways 1. Inflammation of the airway mucosa 2. Hyperplasia of the mucous glands and goblet cells 3. Contraction of smooth muscles - bronchospasm 4. Loss of elasticity of airway wall and lung tissue, airway remodelation
C. Lung parenchyma 1. Emphysema 2. Post – inflammatory (postinjury) fibrosis 3. Interstitial infiltration or fibrosis 4. Intraalveolar processes – pneumonia, alveolar edema.... D. Vascular 1. Pulmonary congestion 2. Pulmonary hypertension E. Pleural 1. Pleural effusions, inflammations 2. Pleural scaring 3. Pneumothorax, hydrothorax...
Alveolar volumes and gravity Different alveolar volume depends on different transpulmonary pressure and Elasticity curve of alveolar unit
Regional differences in alveolar ventilation Elasticity curve of the alveolar unit
Distribution of air in lungs and mechanisms involved in its disturbances - Distribution of alveolar volume - depends on mechanical characteristics and the force (transpulmonaly pressure) exerted on different part of lungs and different alveolar units (inflammation, fibrosis, emphysema, gravity,degree of lung inflation, breathing phase) during breathing - It is clear that underpathological conditions the alveolar volume distribution is profoundly disturbed, is unequal - Distribution of alveolar ventilation - depends on the same factors as distribution of alveolar volume, and is unequal, too
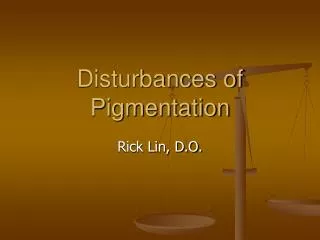
Changes in alveolar volume distribution and in alveolar ventilation distribution may lead to 4 possible situations • Equal distribution of volume andventilation-VA and VA are of the • same magnitude in all alveoli equal distribution oftheVA/VA ratio • (ideal situation) b)Distribution of VA and VAin the lung is unequal, but they have the same proportion in the same compartment Note !Equality of the VA/VA ratio in each alveolar unit of the lung is more important for the gas exchange than equality in total magnitude of the mentioned separate components in the lungs
c)Unequal distribution of ventilation ( VA1 VA2 ) is accompanied by equal distribution of volume (VA1= VA2) Common situation - even under normal condition there are regional differences in the VA/VA ratio as a result of the effect of gravity on the lung -some alveolar units – small amount - may be sligtly hypo- or hyperventilated under these conditions d)Unequal distribution of volume (VA1 VA2) accompaniedby equal distribution of ventilation (VA1=VA2) This type of unequality is not common (some-large amount of alveolar unit may be hypoventilated, other hyperventilated) Disturbances of alveolar volume and alveolar ventilation distribution may be space and time dependent. Very often can beseen unequal and asynchronous ventilation
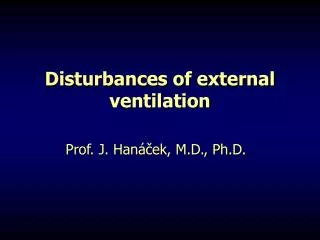
A B VA 1 2 1 2 VA VA VA1= VA2 VA1< VA2 VA1= VA2 VA1< VA2 VA1/VA1 = VA2/VA2 VA1/VA1 = VA2/VA2 C D 2 1 1 2 VA1< VA2 VA1= VA2 VA1< VA2 VA1= VA2 VA1/VA1 > VA2/VA2 VA1/VA1 < VA2/VA2
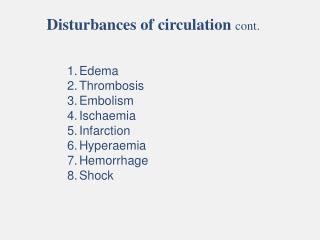
Differences in regional flow resistance in airways as a cause • of unequal and asynchronous ventilation • (In previous figure – part A) - Raw 1(airway resistance in compartment 1) is higherthan Raw 2 • If C1(compliance in compartment 1) is the same as in C2– ventilation of • compartment 2 is higher than in compartment 1. Compartment 1 ventilation also • legs in time behind compartment 2,i.e. besides inequality thereis also • asynchrony of ventilation • Inequality and asynchrony increase with rate of breathingbecause airway • resistance in the place of airway stenosis increases with rate of breathing. This • situation can occur in obstructive types of lung diseases(asynchronous and • uneven alveolar ventilation) • Slow, deep breathing is thus favourable in cases ofobstructive type of • lung diseases
2. Differences in the elasticity of the lung distributionas a cause of unequal and asynchronous ventilation(In figure – part B) • CL( decreased lung compliance) not equally distributedover the whole lung • leads to asynchronous and uneven alveolar ventilation • C1is lower than C2 (because, e.g. fibrosis in compartment 1),ventilation of • compartment 1 is lower than compartment 2, and besides inequality there is • asynchrony: the ventilation ofthe diseased part of alveolar units precedes • that of the normal parts of lung • The opposite of what happens in obstructive lung disease, incases of disturbances • of elasticity, the limiting factor foralveolar ventilation is not the rate of • breathing but the breathing volume. In these conditions, shallow, rapid • breathing is more effective
2 1 A RC1 > RC2 B VA1/VA1 < VA2/VA2 CL VA Raw 2 1 VA1 VA2 RC1 < RC2 VA1/VA1 < VA2/VA2 2 VT 2 1 1 time
Pathological processes involved in disturbances in distribution of air in the lung I. Extrapulmonary causes A. Peripheral nervous system 1. Polyneuritis in one - side of the chest 2. Trauma influencing nervous system in one side of the body (one-side phrenic nerve damage ....) B.One - side primary and secondary myopathy C. Kyphoscoliosis, trauma or surgery of one - side of the chest
II. Pulmonary causes : • Unevenly distributed obstruction of the peripheral bronchi 1. Inflammation of airway mucosa 2. Hyperplasia of the mucous glands and goblet cells 3. Bronchospasm 4. Loss of elasticity of airway wall, airway remodelation B. Uneven distribution of lung parenchyma damage 1. Emphysema 2. Post - inflammatory fibrosis 3. Intersticial infiltration or fibrosis 4. Intraalveolar processes - pneumonia
C. Vascular changes unevenly distributed : 1. Pulmonary congestion 2. Pulmonary edema D. Pleural changes unevenly distributed 1. Pleural effusions, inflammations 2. Pleural scaring 3. Pneumothorax
Diffusion of gases across the A –c membrane and its disturbances Diffusion of gases in the lung is a passive process Components of alveolar - capillary diffusion 1. Membrane factor- transport of gases across the membrane is determined by the following factors : a)alveolar-capillary gas pressure gradient b)solubility and molecular weight of the gases c) thickness, surface area and composition of the A-c membrane} represented bydiffusion coefficient
2. Blood factor- binding of gases to the haemoglobin is determined by: a) rate at which the gas combines with haemoglobin b) capillary blood volume c) venous - capillary gas pressure gradient 3.Circulatory factor- the transport of the dissolved gases with the circulation depends on the following factors : a) capacitance coefficient b) blood flow in the alveolar capillaries c) arterial- venous gas pressure gradient
Lung diffusion capacity = Lung transfer factor =amount of gas (in mmol) diffused across the alveolar – capillarymembraneduring 1 min at the pressure difference 1 kPa Transfer coefficient= transfer factor per 1l of VA a) Alveolar- capillary transport of carbon dioxide and its disturbances - Carbon dioxide - diffuses very easy across alveolar - capillary membrane because of high solubility of CO2 - Limiting factor in CO2 exchange is thus blood factor, and circulatory factor is also important
Under normal conditions at rest there is no measurable Pco2 • gradient between the alveolar gas and the gas at the venularend • of alveolar capillary • In pathological conditions a small alveolar end-capillarygradient of CO2 • can occur (pCO2 in capillary blood). This indicates a serious disturbance • of alveolar-capillarydiffusion or very rapidperfusion ofthe blood in A-c • bed • Even in normal circumstences there is a small A-c CO2 gradient during • physical activity • In lung function disturbances this gradient increases with intensity • of exertion
A PA CO2 PV CO2 PC´ CO2 Er 6 6 45 45 5,4 5,4 40 40 CO2 exchange KPa mmHg KPa mmHg PV CO2 - disturbance excercise rest state C B norm - PA CO2 PC´ CO2 0,8s 0,4s
b)Alveolar - capillary transport of oxygen and its disturbances • Diffusion of O2 across the A-c membrane is limitingfactor because of • relatively bad solubility of O2 in fluids • Other limiting factors in O2 exchange are blood factor andcirculating • factor - Neither at rest nor during work there is an oxygen gradient between the alveolar gas (A) and the end - capillary blood (c) in healthy persons
B) Thenormal alveolar - arterial gradient in O2 is almost entirely the result of venous mixing or of unequal ventilation - perfusion ratios B) During work, the inequality in ventilation-perfusion ratio diminishes C) In various lung function changes the A-c trasport of O2 is disturbed, bringing about an abnormally large oxygengradient between the alveoli and the end-capillary blood D) Under hypoxic conditions the alveolar tension of O2 is low O2 flows across the membrane more slowly and the rate at whichO2 combines to Hb is than too low for equilibrium to be created betweenthe alveolar gas and the capillaryblood before the blood leaves the pulmonary capillaries
100 100 100 12 12 12 40 40 40 4 4 4 0,8 s 0,4 s 0,8 s A PA O2 PV O2 PC´ O2 KPa mmHg PC´ O2 ~ PA O2 rest state norm - KPa mmHg B - disturbance D PA O2 PV O2 PC´ O2 PC´ O2 ~ PA O2 hypoxia PC´ O2 C PV O2 exercise PV O2
Pathological processes involved in disturbances of A – c gas transport A.Normal A-c membraneisuniform in structure The major portion of A-c surface is effectively involved in gas exchange B. The increase in pulmonary blood flow– e.g. physical exertion: - number of functioning capillaries effective surface areaof A-c membrane transfer factor and coefficient C.Pathological processes in the A-c membrane(inflammation, fibrosis, edema, embolism):the gas transfer properties are reduced and distributed unequally. The transfer factor and coefficient are abnormally low
D.Local loss of function of the lung tissue(atelectasis, tumours, inflammation, resection): the effective alveolar surface is small, where as transfer in the remaining normal alveoli may not be disturbed transfer factor is decreased, transfer coefficient in undamaged lung tissue is usually normal E.Obstruction in the pulmonary circulation(e.g. stenosis of mitral valve): the blood volume per alveolus increases,filling of the capillaries is greater and hitherto closed capillaries will open. This is associated with a decrease in pulmonary blood flow transfer factor and transfer coefficient
F.In emphysema : effective A-c surface area transfer factor transfer coefficient G.Abnormal haemoglobin (Hb) molecule (e.g. methaemoglobin) or abnormal quantity of Hb (anemia, polycythemia) influence the A-c gas transfer H.Thickening of A-c membrane( quantity of intersticial fluid, interstitial alveolar fibrosis, primary pulmonary hypertension) disturbances of gas transfer I.Pulmonary edema: distance for gas diffusion gas transfer transfer factor and transfer coefficient
C B A D F E G I H
Perfusion of lung by blood and its disturbances Pulmonary circulation- low pressure system (BP is about (functional)1/5 - 1/7 of that in systemic circulation) • the most important function of the pulmonary • circulation is the exchange of gases Nutritional pulmonary circulation- bronchial arteries - high pressure system. Capillaries of functional pulmonary circulation anastomose with nutritional ones. For more information on pulmonary circulation look at textbook of physiology !
Regional lung perfusion and gravity With regard to the alveolar vessels (not extraalveolar vessels)West has created a model in which the lung is divided into4zones: Zona 1:Pericapillary pressure (Ppc) exceeds the pressure in the pulmonary artery and vein. Ppc is slighthy smaller thanthe alveolar (atmospheric) pressure.Blood flow across this zone is low or absent Zona 2:Pulmonary arterial pressure (Ppa) is greater than the Ppc, which in turn is greater than the venous bloodpressure. Blood flow is determined by difference between Ppa-Ppc. The intracapillary and pericapillary pressures are almostthe same. Blood flow is present
Zona 3: Ppc is below the arterial and venous pressure and the blood flow is determined by the arterial - venous pressure gradient. This results in greater capillaryfilling (capillary distension) and increased blood flow through capillaries. Blood flow is there the highest comparing with other zones of the lung Zona 4 :Try to explain the mechanisms influence the blood flow across this zone !
Pathological processes involved in disturbances ofblood perfusion across the lung A change in lung perfusion is the result of a change in the degree of filling and/or the number of capillariesinvolved in the perfusion A.Normal perfusionin a sitting position at rest: perfusion of basal parts of the lung is considerable, while apicalzone is perfused, but little B.Increased perfusion during work: apical zone is perfused and regional differences are still present but in lower intensity. Intensity of regional blood flow differences depends on intensity of exercise
C.Greatly increased perfusion: caused by heavy work orsevere cardiac left - right shunt. Regional differences in blood flow are not present D.Decreased perfusion:caused by pulmonary hypotension or other causes leading to reduced cardiac output (e.g. embolisation to pulmonary artery) E.A reduced capillary bed:due to destruction of capillaries (inflammation, degeneration, vascular obstruction, emphysema, tumours ) totally unequal perfusion F.Capillary blockage:is caused by obstruction of venous return (e.g. left heart failure)