Analysis and presentation of Case-control study data
Analysis and presentation of Case-control study data. Chihaya Koriyama February 14 (Lecture 1). Study design in epidemiology. Why case-control study?.

Analysis and presentation of Case-control study data
E N D
Presentation Transcript
Analysis and presentation of Case-control study data Chihaya Koriyama February 14 (Lecture 1)
Why case-control study? • In a cohort study, you need a large number of the subjects to obtain a sufficient number of case, especially if you are interested in a rare disease. • Gastric cancer incidence in Japanese male: 128.5 / 100,000 person year • A case-control study is more efficient in terms of study operation, time, and cost.
Comparison of the study design Case-control Cohort Rare diseases suitable not suitable Number of disease 1 1< Sample size relatively small need to be large Control selection difficult easier Study period relatively short long Recall bias yes no Risk difference no availableavailable
Case-control study - Sequence of determining exposure and outcome status • Step1: Determine and select cases of your research interest • Step2: Selection of appropriate controls • Step3: Determine exposure status in both cases and controls
Case ascertainment • What is the definition of the case? • Cancer (clinically? Pathologically?) • Virus carriers (Asymptomatic patients) → You need to screen the antibody • Including deceased cases? • You have to describe the following points, • the definition • when, where & how to select
Who will be controls? • Control ≠ non-case • Controls are also at risk of the disease in his(her) future. • “Controls” are expected to be a representative sample of the catchment population from which the case arise. • In a case-control study of gastric cancer, a person who has received the gastrectomy cannot be a control since he never develop gastric cancer .
Various types of case-control studies 1)a population-based case-control study Both cases and controls are recruited from the population. 2)a case-control study nested in a cohort Both case and controls are members of the cohort. 3)a hospital-based case-control study Both case and controls are patients who are hospitalized or outpatients. Controls with diseases associated with the exposure of interest should be avoided.
The following points should be recorded (described in your paper) • The list (number) of eligible cases whose medical records unavailable • The list (number) of refused subjects, if possible, with descriptions of the reasons of refusal • The length of interview • The list (number) of subjects lacking the measurement data, with descriptions of the reasons
Exploratory or Analytic • Exploratory case-control studies • There is no specific a priori hypothesis about the relationship between exposure and outcome. • Analytic case-control studies • Analytic studies are designed to test specific a priori hypotheses about exposure and outcome.
Case-control study - information • Sources of the information of exposure and potential confounding factors • Existing records • Questionnaires • Face-to-face / telephone interviews • Biological specimens • Tissue banks • Databases on biochemical and environmental measurements
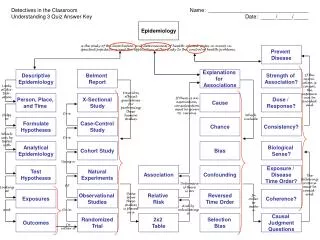
Temporality is essential in Hill’s criteria The study exposure is unlikely to be altered at this stage because of the disease. The study exposure is more likely to be altered at this stage because of the symptoms. Essential Epidemiology (WA Oleckno)
Bias should be minimized • Bias & Confounding • Selection bias • Detection bias • Information bias (recall bias) • Confounding Confounding can be controlled by statistical analyses but we can do nothing about bias after data collection.
Case-control studies ・・・ • are potential sources of many biases • should be carefully designed, analyzed, and interpreted.
How can we solve the problem of confounding in a case-control study? “Prevention” at study design • Limitation • Matching in a cohort study But not in a case-control study
Matching in a case-control study • Matched by confounding factor(s) to increase the efficiency of statistical analysis • Cannot control confounding • A conditional logistic analysis is required.
Over matching • Matched by factor(s) strongly related to the exposure which is your main interest • CANNOT see the difference in the exposure status between cases and controls
How can we solve the problem of confounding? “Treatment “ at statistical analysis • Stratification by a confounder • Multivariate analysis
What you should describe in the materials and methods, • Study design • Definition of eligible cases and controls • Inclusion / exclusion criteria of cases and controls • Number of the respondents and response rate • Main exposure and other factors including potential confounding factors
What you should describe in the materials and methods, • Sources of the information of exposure and other factors • Matched factors, if any • The number of subjects used in statistical analyses • Statistical test(s) and model(s) • Name and version of the statistical software
Assuring adequate study power • Following information is necessary • The confidence level desired (usually 95% corresponding to a p-value of 0.05) • The level of power desired (80-95%) • The ratio of controls to cases • The expected frequency of the exposure in the control group • The smallest odds ratio one would like to be able to detect (based on practical significance)
Statistical analysis “Matched” vs. “Unmatched” studies The procedures for analyzing the results of case-control studies differ depending on whether the cases and controls are matched or unmatched. Matched Unmatched ・McNemar’s test ・Chi-square test ・Conditional logistic ・Unconditional logistic regression analysis regression analysis
Advantages of pair matching in case-control studies • Assures comparability between cases and controls on the selected variables • May simplify the selection of controls by eliminating the need to identify a random sample • Useful in small studies where obtaining cases and controls that are similar on potentially confounding factors may otherwise be difficult • Can assure adequate numbers of subjects with specified characteristics so as to permit statistical comparisons Essential Epidemiology (WA Oleckno)
Disdvantages of pair matching in case-control studies • May be difficult or costly to find a sufficient number of controls • Eliminates the possibility of examining the effects of the matched variables on the outcome • Can increase the difficulty or complexity of controlling for confounding by the remaining unmatched variables • Overmatching • Can result in a greater loss of data since a pair of subjects has to be eliminated even if ne subject is not responsive Essential Epidemiology (WA Oleckno)
An example of unmatched case-control study Lung cancer Controls cases N=100 N=100 Smokers (NOT recently started) ↓ ↓ 70 40 Odds ratio=
Risk measure in a case-control study Odds = prevalence / (1- prevalence) Odds ratio = odds in cases / odds in controls Disease +(case) -(control) + a c Exposure - b d Exposure odds in cases =a / b Exposure odds in controls=c / d Odds ratio=(a / b) / (c / d) = a * d / b * c
An example of matched case-control study Lung cancer Matched controls Cases by sex & age N=100 N=100 Smokers (NOT recently started) ↓ ↓ 70 40 Notice that this is the distribution of 100 matched pairs.
McNemar’s test Chi-square (test) statistic = (40 – 10)2 / (40+10) = 18 where degree of freedom is “1”. Odds ratio = 40 / 10 = 4
Logistic regression analysis • Logistic regression is used to model the probability of a binary response as a function of a set of variables thought to possibly affect the response (called covariates). 1: case (with the disease) Y = 0: control (no disease)
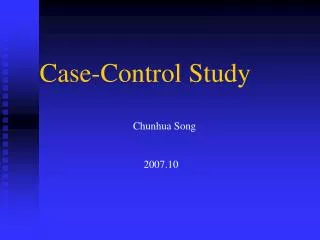
One could imagine trying to fit a linear model (since this is the simplest model !) for the probabilities, but often this leads to problems: In a linear model, fitted probabilities can fall outside of 0 to 1. Because of this, linear models are seldom used to fit probabilities. Probability
In a logistic regression analysis, the logit of the probability is modelled, rather than the probability itself. P = probability of getting disease p logit (p) = log 1-p As always, we use the natural log. The logit is therefore the log odds, since odds = p / (1-p)
Simple logistic regression (with a continuous covariate) Suppose we give each of several beetles some dose of a potential toxic agent (x=dose), and we observe whether the beetle dies (Y=1) or lives (Y=0). One of the simplest models we can consider is to assume that the relationship of the logit of the probability of death and the dose is linear, i.e., px logit (px) = log = a + b x 1 – px where px = probability of death for a given dose x, and a and b are unknown parameters to be estimated from the data.
The values of a and b will determine whether or not and how steeply the dose-response curve rises (or falls) and where it is centered. If b = 0 px is constant over x b > 0 px increases with x b < 0 px decreases with x H0: b = 0 is the null hypothesis in a “test of trend” when x is a continuous variable. Knowledge of b would give us insight to the direction and degree of association outcome and exposure. e (a+bx) Px = 1 + e (a+bx)
Simple logistic regression (with a dichotomous covariate) Suppose we are considering a case-control study where the response variable is disease (case) / non-disease (control) and the predictor variable is exposed / non-exposed, which we “code” as an indicator variable, or dummy variable. 1 D1 1 E1 Y = x = 0 D0 0 E0 And px = Prob (disease given exposure x) = P (Y = 1 | x) x = 0, 1 Thus, p1 = probability of disease among exposed p0 = probability of disease among non-exposed
In case of exposure (X=1): logit(PE1)=intercept + b In case of non-exposure (X=0): logit (PE0) =intercept If you want to obtain odds ratio of exposure group, OR=(PE1 / (1-PE1))/ (PE0 / (1-PE0)) log(OR) = log {(PE1 / (1-PE1))/ (PE0 / (1-PE0))} = log (PE1 / (1-PE1)) – log(PE0 / (1-PE0)) = logit (P for exposure) – logit (P for non-exposure) = (intercept + b) – intercept = b Definition of odds ratio OR = e b
Simple logistic regression(with a covariate having more than two categories) Suppose we are considering a case-control study where the predictor variable is current smoker / ex-smoker / non-smoker, which we “code” as a dummy variable. Original data Dummy variables
Logistic regression model of the previous example logit (P) = a + b1(X1) + b2 (X2) In case of current smoker (X1=1, X2=0): logit(Pcurrent)= a + b1 In case of ex-smoker (X1=0, X2=1) : logit(Pex)= a + b2 In case of non-smoker (X1=0, X2=0) : logit(Pnon)= a ORcurrent = e b1 ORex = e b2 ORnon = 1 (referent)
Wald’s test for no association The null hypothesis of no association between outcome and exposure corresponds to H0: OR=1 or H0: b =logOR=0 Using logistic regression results, we can test this hypothesis using standard coefficients or Wald’s test. Note: STATA and SAS present two-sided Wald’s test p-values.
Likelihood Ratio Test (LRT) An alternative way of testing hypotheses in a logistic regression model is with the use of a likelihood ratio test. The likelihood ratio test is specifically designed to test between nested hypotheses. H0: log (Px / (1-Px)) = a HA: log (Px / (1-Px)) = a + bx and we say that H0 is nested in HA.
Likelihood Ratio Test (LRT) In order to test H0 vs. HA, we compute the likelihood ratio test statistic: G= -2・log(LH0 / LHA) = 2 (log LHA – log LH0) = (-2log LH0) – (-2log LHA) Where LHA is the maximized likelihood under the alternative hypothesis HA and LH0 is the maximized likelihood under the null hypothesis H0. If the null hypothesis H0 were true, we would expect the likelihood ratio test statistic to be close to zero.
Wald’s test vs. LRT • In general, the LRT often works a little better than the Wald test, in that the test statistic more closely follows a X2 distribution under H0. But the Wald test often works very well and usually gives similar results. • More importantly, the LRT can more easily be extended to multivariate hypothesis tests, e.g., • H0: b1 = b2 = 0 vs. HA: b1 = b2 = 0
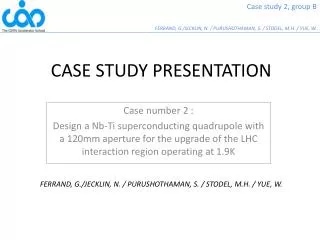
RECURRENT CASES LIVED IN VALLE DEL CAUCA LESS THAN 5 YEARS PATIENTS NEWLY DIAGNOSED AS G.C. 395 65 16 7 Sep.2000~ Dec.2002 91 REFUSED TO PARTICIPATE IN THE STUDY COULD NO CONTACT Recruitment of cases 81 cases were excluded 2 173 formalin-fixed paraffin-embedded blocks 1 216 CASES 4 3 We could not obtain the information on tumor location for 23 cases, and those cases were excluded from the tumor location specific analysis.
LIVED IN VALLE DEL CAUCA LESS THAN 5 YEARS REFUSED TO PARTICIPATE IN THE STUDY 67 29 1 Histry of G.C. Recruitment of controls 1 Matched by sex, age (5-year ), hospital, date of administration Case: control= 1 : 2 2 POTENTIAL CONTROLS 528 431 CONTROLS 3 Major diseases of controls • cardiovascular diseases (208) • trauma (117) • infectious diseases (38) • urological disorders (21)
| gastric cancer Smoking | 0 1 | Total -----------+----------------------+---------- Never 0 | 188 78 | 266 Ex- 1 | 145 89 | 234 Current 2 | 98 49 | 147 -----------+----------------------+---------- Total | 431 216 | 647 xi:logistic casocon i.fumar i.fumar _Ifumar_0-2 (naturally coded; _Ifumar_0 omitted) Logistic regression Number of obs = 647 LR chi2(2) = 4.24 Prob > chi2 = 0.1198 Log likelihood = -409.93333 Pseudo R2 = 0.0051 ------------------------------------------------------------------------------------------------ casocon | Odds Ratio Std. Err. z P>|z| [95% Conf. Interval] -------------+---------------------------------------------------------------------------------- _Ifumar_1 | 1.479399 .2817549 2.06 0.040 1.018526 2.148813 _Ifumar_2 | 1.205128 .2660901 0.85 0.398 .7817889 1.857706 ------------------------------------------------------------------------------------------------ Walt’s test p values
Results of conditional logistic regression analysis using the same data Case Control OR (95%CI) Fumar=0 Fumar=1 Fumar=2 xi:clogit casocon i.fumar, group(identi) or Conditional (fixed-effects) logistic regression Number of obs = 647 LR chi2(2) = 4.64 Prob > chi2 = 0.0982 Log likelihood = -234.5745 Pseudo R2 = 0.0098 --------------------------------------------------------------------------------------------------- casocon | Odds Ratio Std. Err. z P>|z| [95% Conf. Interval] -------------+------------------------------------------------------------------------------------- _Ifumar_1 | 1.535023 .3061998 2.15 0.032 1.038295 2.269389 _Ifumar_2 | 1.219851 .2784042 0.87 0.384 .7799 1.907985 --------------------------------------------------------------------------------------------------- Wald’s test p values Stata command
P = 0.51 GC risk by smoking in Cali, Colombia results of tumor-location specific analysis P value by LRT This test examines the difference in the magnitude of the association between smoking and GC risk among 3 tumor sites.