Download
1 / 15
150 likes | 342 Vues
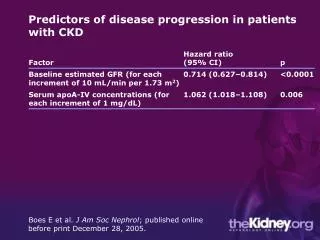
CLINICAL PRESENTATION AND PREDICTORS OF OUTCOME IN PATIENTS WITH SEVERE ACUTE EXACERBATION OF COPD REQUIRING ADMISSION TO ICU By Mohan et al. BACKGROUND. COPD is a common, costly preventable disease and is the 4 th leading cause of death globally

E N D
CLINICAL PRESENTATION AND PREDICTORS OF OUTCOME IN PATIENTS WITH SEVERE ACUTE EXACERBATION OF COPD REQUIRING ADMISSION TO ICUBy Mohan et al
BACKGROUND • COPD is a common, costly preventable disease and is the 4th leading cause of death globally • Acute exacerbation of COPD(AE-COPD) is a common cause of ER visit • Major cause of morbidity and mortality with more than half of these patients requiring re-admission in subsequent 6 months • Great variability in clinical course making predictions of outcome in a given patient difficult • The study was designed to prospectively study the clinical presentation and predictors of outcome in patients with AE-COPD requiring admission to ICU
METHODS • During period from June 2000 and December 2004 , 914 patients diagnosed with COPD in MOPD and Chest Clinic at a Tertiary Hospital • 314 of these later on presented to ER with AE-COPD • After appropriate initial treatment, 116 admitted to Medical ICU, 18 discharged, 180 admitted to Acute Medical Unit and Medical Ward • Basis of study is on the 116 admitted to ICU • Patients with bronchiectasis, interstitial lung disease,PE, Pulmonary Oedema excluded • Study was approved by Ethical Committee
COPD diagnosed on basis of Pulmonary Function tests during MOPD visits • AE-COPD diagnosed if all following present: rapid worsening dyspnoea, increase in sputum volume and purulence • Only single enrolement per patient regardless of frequency of exacerbations • On arrival full Hx including type of smoking habit cigarette or bidi and pack years, domestic fuel use and examination • Baseline investigations including imaging
O2 given as appropriate nasal prongs, face mask or Ventura devices • Nebs of Salbutamol/Ipratropium every 15 min to 8 hourly , steroids if no improvement iv aminophylline. Empiric antibiotics given could be changed on sensitivities • No standard criterion for Invasive Ventilation • In study indications include, failure to respond to pharmacologic and other non-ventilatory Rx, severe dyspnoea, severe acidosis (pH < 7,25) , hypercapnea (P CO2 > 60mmHg), life threatinghypoxaemia, respiratory arrest, somnolence, impaired mental status and co-morbid illness
STATISTICAL ANALYSIS • Variables following normal distribution were summarised by mean and standard deviation • Association between two categorical variables was by χ2 or Fisher’s exact test as appropriate • Student t test used for quantitative variables • Quantitative variables categorised and if it showed statistically significant association with outcome at p < 0.20 considered for inclusion • Stepwise multivariate logistic regression performed with potential candidate variables as co-variates • SYSTAT Version 7.0 used. All stat tests performed were two tailed, p <0.05 considered statistically significant
RESULTS . Mean age 62.1 ± 9.8 years with 102(88%) males .Mean duration of COPD 7.2 ± 5.8 years .All males were smokers for 22.3 ± 11.2 pack years 35.2% smoked cigarettes and 64.8 % smoked bidis. All women non-smokers and were exposed to domestic fuels .81 (69.8%) patients had co-morbid illness with 53 (45.7%) having one condition and 28(54.3%) having 2 or more .Past PTB in 33(28.4%) patients, 5 patients with Type 2 DM found to have active PTB .ABG showed Respiratory Failure in 40(33.8 %) patients Type 1 in 17.5% and Type 2 in 82.5% .Invasive Ventilation required in 18 patients .16 (13.7%) patients died in the study Predictors of death: need for invasive ventilation, presence of co-morbid illness and hypercapnoea
Table 1 Demographic characteristics and co-morbid conditions in 116 patients with acute exacerbation of chronic obstructive pulmonary disease admitted to the medical intensive care unit • GOLD = Global Initiative for Chronic Obstructive Lung Disease (reference 1) • COPD = chronic obstructive pulmonary disease • * In all patients post-bronchodilator forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) was ≤ 0.7. Moderately severe COPD, FEV1 = 50 – 80% predicted; severe COPD, FEV1 = 30 – 50% predicted; very severe COPD = <30% predicted (reference 1) • † 3 patients had diabetic ketoacidosis and 5 patients had active pulmonary tuberculosis • ‡ Clinical and radiographic evidence of past tuberculosis was present • More than one co-morbid conditions were present in several patients • Mohan et al.BMC Pulmonary Medicine 2006 6:27 doi:10.1186/1471-2466-6-27
Table 2 Clinical presentation in 116 patients with acute exacerbation of chronic obstructive pulmonary disease admitted to the medical intensive care unit • JVP = jugular venous pulse • Mohan et al.BMC Pulmonary Medicine 2006 6:27 doi:10.1186/1471-2466-6-27
Table 3 Laboratory abnormalities in 116 patients with acute exacerbation of chronic obstructive pulmonary disease admitted to the medical intensive care unit • ESR = erythrocyte sedimentation rate • Mohan et al.BMC Pulmonary Medicine 2006 6:27 doi:10.1186/1471-2466-6-27
Table 4 Predictors of outcome in 116 patients with severe acute exacerbation of chronic obstructive pulmonary disease requiring admission to the intensive care unit: univariate sensitivity analysis • Mohan et al.BMC Pulmonary Medicine 2006 6:27 doi:10.1186/1471-2466-6-27
Table 5 Predictors of death in 116 patients with severe acute exacerbation of chronic obstructive pulmonary disease requiring admission to the intensive care unit: stepwise multivariate logistic regression analysis • Mohan et al.BMC Pulmonary Medicine 2006 6:27 doi:10.1186/1471-2466-6-27
DISCUSSION • Not much info on burden of AE-COPD in ER, its presentation and outcome • Significant number of patients (n=53; 45.7%) had co-morbid conditions, and this was a predictor of death • Accurate assessment of co-morbid conditions and institution of specific treatments should help to reduce morbidity and mortality • Past PTB important cause of COPD and also of AE-COPD (p<0.001) • Ramifications in areas where PTB endemic and smoking on the rise • High prevalence of respiratory failure in study . Invasive ventilation associated with poor prognosis • In conclusion, in addition to host genetic factors, smoking behaviour, accessibility to health care and presence of co-morbid conditions contribute to morbidity and mortality due to AE-COPD