Download
1 / 36
360 likes | 671 Vues
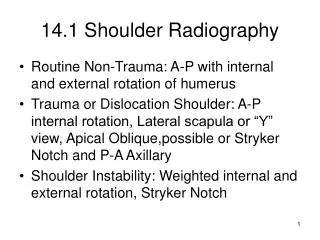
What do accoucheurs really know about the management of Shoulder Dystocia ?. Tim Draycott, Consultant Obstetrician & Gynaecologist. Declaration of Interest. Limbs & Things collaboration Erbs Palsy Group. BBC Shoulder Dystocia. Shoulder Dystocia. Unpredictable → Unpreventable Rare

E N D
What do accoucheurs really know about the management of Shoulder Dystocia ? Tim Draycott, Consultant Obstetrician & Gynaecologist
Declaration of Interest Limbs & Things collaboration Erbs Palsy Group
Shoulder Dystocia • Unpredictable → Unpreventable • Rare • Some fetal morbidity may be due to inappropriate/inadequate management • OBPI complicates 4-16% SD deliveries • UK Incidence 1/2300 live birth • Approx 252 per year in UK • No change over last 40 years Evans Jones et al. Arch Dis Child Fetal: 2003
Res ipsa loquitur • “…all brachial plexus injuries are the fault of the accoucheur, who must have applied excessive traction during difficult delivery of the shoulders…” • Incompetence by Incompetents ! • Refuted by medical practitioners
But ………. • In 66% of neonatal deaths after SD, different management may have altered the outcome CESDI 5th Annual Report - Focus Group Shoulder Dystocia, London • 42% Staff did not feel confident to manage SD Neil et al, Shoulder dystocia: room for improvement? J Obs Gynae 1999
What do we really know ? SaFE Study • 6 Hospitals • 141 Staff • 96 Midwives • 45 Doctors
SaFE Study Design Pre-training Assessment Training Intervention Post-training Assessments 3 weeks, 6 months and 12 months
Evaluation of training • Knowledge - MCQ • Clinical skill - simulation • Shoulder Dystocia • Eclampsia • PPH • Team work - Teamwork Assessment tool (Weller) • Pre & Post training with follow up at 6 months and 1 year
Pre - Basic Manoeuvres Pre-training 81.4% could perform all basic manoeuvres
Pre - Achieved Delivery Pre-training 42.9% could deliver the baby
Observed Difficulties 450 consecutive simulated deliveries • Inability to gain vaginal access to perform internal manoeuvres • Confusion over internal rotational manoeuvres • Attempting to deliver the posterior shoulder NOT the posterior arm • Requesting fundal pressure and applying supra-pubic pressure
What we don’t know ? Knowledge • 46 % unaware fundal pressure could cause uterine rupture Skills • 16% could not perform basic actions • 57 % could not do more than McRoberts & SPP • 66% pulled above 100 N • 4% performed fundal pressure
Why deficiencies ? • Not bad practitioners, but poor training • Difficult to train • Accurate models • Syllabus • How best to train
Accurate Models ? • “The most bio-fidelic model available.” R. Allen. Johns Hopkins University, Baltimore. 2002
Noelle Compared with no training (n=17) • Timeliness of intervention • Overall performance • Decreased head-to-body time Deering et al, Improving resident competency in the management of shoulder dystocia with simulation training. AJOG 2004 6 p1224-8
SaFE Study Results • Increase in delivery rate • 43.9% v 83.3% (p<0.001) • Reduction in total force • 2,030Ns v 2,916Ns (p=0.009) • Number of participants with good communication (score ≥ 4) increased • 56.8% to 82.6% (p<0.001)
Conclusions • High Fidelity mannequin – L&T • Improved delivery rate (72% vs 89%) • Improved performance of int. manoeuvres • Reduction in peak force of 10N • Significantly less called for Paed Crofts, Draycott et al. Obstet Gynecol. 2006
SD at Southmead New Training Training on high fidelity mannequin Introduced 2000 100% staff annual updates 70% reduction of neonatal injury post training (p<0.001)
Injuries after SD *RR=0.27 *p<0.0001 (Chi-squared test)
New Problem ? “The course no sooner finished, [these] young surgeons and women, rushing to benefit from a profession they know only superficially. But when difficulties arise they are absolutely unskilled, and until long experience instructs them they are the witness or the cause of many misfortunes, of which the least terrible is the death of the mother or the child and even both..” Madame du Coudray to Louis XV 1756
M du Coudray 1756 • Obstetric Machine
Conclusion • Verified a training need • Pre-training knowledge and skills deficiencies • Possibly upto 70% of injuries may be avoidable • Training improves performance • High fidelity trainer offers some advantages • Error reduction can directly improve perinatal outcome
Thankyou All staff in SW SaFE Study Team PROMPT training programme tdraycott@gmail.com safestudy@hotmail.com