Download
1 / 21
210 likes | 333 Vues
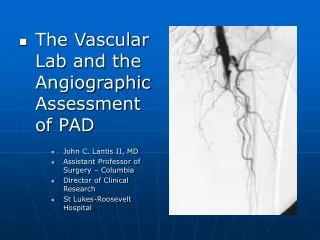
The Vascular Lab and the Angiographic Assessment of PAD John C. Lantis II, MD Assistant Professor of Surgery – Columbia Director of Clinical Research St Lukes-Roosevelt Hospital. The Questions. Does the patient have enough blood flow to heal their wound / or the intervention ?

E N D
The Vascular Lab and the Angiographic Assessment of PAD • John C. Lantis II, MD • Assistant Professor of Surgery – Columbia • Director of Clinical Research • St Lukes-Roosevelt Hospital
The Questions • Does the patient have enough blood flow to heal their wound / or the intervention ? • Does the patient have PAD, and should I be helping them to find coordinated care ? • Is the patients circulation compromised to the point that I am highly concerned about tissue loss ?
The Answers! • (Obviously) A good physical exam • Physiologic testing • Ankle brachial index • Pulse volume recording • Duplex/MRI – NOVA • TCPO2 (Transcutaneous Oxygen Tension) • Anatomic testing • Duplex • MRA • Angiogram • CTA
The Ankle Brachial Index • Measurement of segmental leg pressure compared to the highest brachial artery pressure • Can be done at the bedside • Requires little equipment • Helps determine level of disease
The ankle brachial Index • Prognostic capabilities • Forefoot amputations are likely to heal, if the ankle pressure is > 70 mmHg, or if the ABI > 0.45 • Toe amputations are likely to heal with ankle pressures of > 35 mmHg or toe pressures > 55 mmHg • Limitations • Ankle pressures can be artificially inflated in patients with diabetes mellitus and ESRD • Toe pressures are therefore relied upon • Pressure less than 50 mm Hg and a toe-to-arm ratio of less than 0.6 is indicative of ischemic arterial disease • Foot lesions usually heal if toe pressures exceed 30 mmHG in non-diabetic patients and 55 mmHG in diabetic patients • Ipsilateral ankle to toe pressures can be used to assess for obstructive pedal vascular disease • AVG 0.65 in normals • AVG 0.23 in patients with rest pain of tissue loss
Pulse Volume Recordings • More sensitive and more specific • Probably the bread and butter physiologic test • Will give good guidance to the level and severity of disease
Pulse Volume Recordings(with ABI and exercise) • Treadmill walking test • Walking at 1.8 mph • 10 % incline • Uncovers more subtle lesions • Especially proximal lesions in the iliac and SFA vessels • A fall in the ABI of 0.2 or a recovery to baseline pressure that is greater than 1 minute is significant
Clinical Description Normal Asymptomatic Mild Claudication (ABI - < 0.7) Moderate Claudication Severe claudication Rest Pain (ABI - < 0.4) Minor Tissue Loss Major Tissue Loss Pressure Criteria Normal Treadmill test Completes test, ankle pressure drops > 20 mmHg, absolute ankle pressure > 50 mmHg Between mild and severe Cannot complete treadmill test and ankle pressure after exercise < 50 mm Hg Resting ankle pressure < 60 mmHG or toe pressure < 40 mmHG Resting ankle pressure less than 40 mmHg or toe pressure less than 30 mmHg Same as minor Categories of Chronic Limb Ischemia
Duplex Ultrasound(Combination of B mode imaging and doppler velocity criteria) • Doppler waveform analysis of the femoral, popliteal and tibial vessels can be carried out • Waveforms are evaluated similarly to the PVR tracings • More accurate at localizing disease than PVRs • Very labor intensive
Transcutaneous Partial pressure of Oxygen • Transcutaneous oxygen (tcPO2) • Reflects the metabolic state of the target tissue • Best for severe ischemia • Heated Clark electrode (very tech dependent, hard to reproduce) • < 20 mmHg – healing failure • > 40 mmHg – healing success • Elevate limb > 300 /3 min – drop > 15 mmHg – healing failure
Other Methods of Assessing Blood Supply • Laser Doppler Velocimetry • A relative index of cutaneous blood flow • With ischemia pulse waves are attenuated, mean velocities are decreased • If mean velocity is > 40 millivolts (mV) and pulse wave amplitude is > 4 mV – associated with healing • NOVA • Non-invasive Optimal Vessel Analysis (NOVA) a non-invasive Magnetic Resonance Imaging (MRI) technique • NOVA provides actual milliliter/minute blood flow data using specialized software analysis of standard MRI phase contrast imaging • Investigational
Back to the Questions…. • Does the patient have enough blood flow to heal their wound / or the intervention ? NO • Does the patient have PAD, and should I be helping them to find coordinated care ? YES • Is the patients circulation compromised to the point that I am highly concerned about tissue loss ? YES
Leads to the next two questions… • Where is the patients lesion? • Segmental Pressures • Segmental PVRs • Long leg duplex • Can I get this patient revascularized? • What type of lesion? • How many and where?
MRA • Non nephrotoxic contrast • No arterial puncture • However, claustrophobia limited • Sensitivity and specificity to level of disease 80-85% • Approximately 85 % concordance with Angiography
Angiography • Usually nephrotoxic dye • Arterial puncture • Done with sedation (few issues with claustrophobia) • Able to intervene at time of procedure • With subtraction capabilities probably able to see post-occluded vessels as well as MRA
CT Angiogram • Approaching MRAs capabilities • Relatively large nephrotoxic dye load • No arterial puncture • Minimal claustrophobia issues • Distal vessel resolution still machine and center dependent
A day in the life…. • A patient limps in… • No palpable pulse… • Small amount of tissue loss • ABI/PVRs are obtained • ….Obtain toe NIFs.. • Pt went onto heal..
Or more likely….. • We have flat line tracings • Which we follow with a anatomic diagnostic …. • Which leads us to our next speakers…