Download
1 / 16
160 likes | 353 Vues
The prevalence of inflammatory cells in non ruptured atherosclerotic plaques. G. Pasterkamp Experimental Cardiology, UMC and Interuniversity cardiology Institute of the Netherlands, Utrecht, The Netherlands Published in part in : Arterioscl Thromb and Vasc Biol 1999;19:54-58. Background.

E N D
The prevalence of inflammatory cells in non ruptured atherosclerotic plaques G. Pasterkamp Experimental Cardiology, UMC and Interuniversity cardiology Institute of the Netherlands, Utrecht, The Netherlands Published in part in : Arterioscl Thromb and Vasc Biol 1999;19:54-58.
Background Plaque rupture and subsequent plaque thrombosis is found to be associated with the presence of inflammatory cells. Davies et al. Br Heart J 1985;53:363-373 Van der Wal et al. Circulation 1994;89:36-44 Moreno et al. Circulation 1994;90:775-778
Question Is the presence of inflammatory cells A- specific for plaque rupture or B- a commonly observed phenomenon in atherosclerotic lesions? What is the prevalence of moderate/heavy local inflammation in non ruptured atherosclerotic lesions?
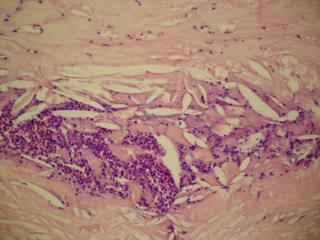
Post mortem study: • Atherosclerotic femoral (n=50) and coronary arteries (n=74) from patients that did not die of cardiovascular disease. • In each artery, 4-6 non ruptured cross-sections revealing atherosclerosis were studied for the presence of macrophages (CD 68) and T-lymphocytes (CD45RO).
positive negative
positive negative
Femoral artery 45% of all cross-sections revealed moderate or heavy staining for macrophages in the cap or shoulder of non ruptured plaques.
Question If one would randomly stain 5-6 cross-sections obtained from an atherosclerotic artery for inflammatory cells, how often would at least one cross-section reveal moderate to heavy staining for inflammatory cells?
positive negative
positive negative
Femoral arteries In 84% of all femoral arteries at least one cross-section revealed moderate or haevy staining for macrophages or T-lymphocytes in cap or shoulder of the non ruptured athertosclerotic plaque.
Question If one would find many cross-sections with inflammation in one coronary artery: would that be predictive for the occurrence of plaque inflammation in another coronary artery? Right and left coronary arteries were compared within the individual (next slide)
-= no staining, + = moderate staining, ++ = heavy staining, No relation was observed between the degree of staining for inflammatory cells between the left and right coronary artery.
Conclusion • The presence of inflammatory cells is a common phenomenon in non ruptured atherosclerotic lesions. • The degree of local inflammation is locally determined and has no/low predictive value for the presence of inflammation in other arteries. (Pasterkamp et al. ATVB 1999, Vink et al JACC 2001)
Discussion • Considering these results: what is the predictive value of local inflammation for the occurrence of plaque rupture? • Visualization of the vulnerable plaque when inflammation is used as marker: • Specificity for local plaque rupture or predictive value for plaque rupture may be disappointing.