Download
1 / 32
340 likes | 366 Vues
Antimicrobial Agents (Sulfonamides and Quinolones). Prof. R. K. Dixit Pharmacology and Therapeutics K.G.M.U. Lucknow dixitkumarrakesh@gmail.com. Objectives. After completion of this lecture you will be able to Know about sulphonamides Types (Classification) MOA

E N D
Antimicrobial Agents (Sulfonamides and Quinolones) Prof. R. K. Dixit Pharmacology and Therapeutics K.G.M.U. Lucknow dixitkumarrakesh@gmail.com
Objectives After completion of this lecture you will be able to • Know about sulphonamides • Types (Classification) • MOA • Combination with Trimethoprim or Pyrimethamine • Uses • ADRs, DDI, and Contraindications • Special points • Know about Quinolones • Types (Classification) • MOA • Uses • ADRs, DDI, and Contraindications • Special points
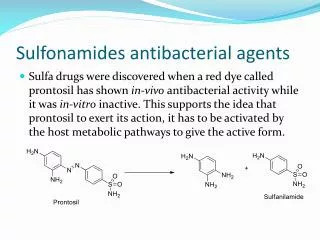
Suphonamides (Sulfonamides) [F=USA, Ph=UK] • First antimicrobial agents effective against bacteria • Prontosil Red (sulfonamide chrysoidine dye) – • by- Domagk – for – streptococcal infection. • Broken down in body – • into- Sulfanilamide (Active against bacteria) • Use increased –Overuse- Development– Resistance • Rarely used (alone) today due to • Availability of safer and effective antibiotics • Resistant
Sulfonamides today used as combination • Trimethoprim (Cotrimoxazole) as antiBacterial • Pyrimethamine (Cotrimazine) as anti-Malarial. TB in PM
Sulfonamides (Chemistry) • Derivatives of • Sulfanilamide (p-Aminobenzene sulfonamide) • Individual member differs in nature of N1substitution. • N1substitution governs- • Pharmacokinetic properties • Free amino group at - (N4)–antibacterial activity. DK- 41
Sulfonamides (Members) • Short Acting (4-8hrs) • Sulfisoxazole • Sulfadiazine- • Less protein bound, • Penetrates BBB- Meningitis • Acetylated product is less soluble and cause for crystalluria • Intermediate acting (8-12 hrs) • Sulfammoxazole • Sulfamethoxazole – • Combination with Trimethoprim, FDC ( Cotrimoxazole) • High fraction is acetylated and may lead to Crystalluria • Long acting (> 12 hrs) • Sulfadoxine - • Very high plasma protein binding and slow renal excretion, • Longest acting, • Used in malaria, Toxoplasmosis, Pneumocystis, • In combination with Pyrimethamine, • Sulfamethoxypyrazine
Special purpose Sulfonamides • Sulfacetamide- • Ocular drops • Mafenide – • Active in presence of • Pus and Pseudomonas • Produces severe burning • Have Carbonic Anhydrase Inhibitor activity • Can alkalinize urine, • Produce Acidosis, & Hyperventilation
Silver sulfadiazine – • Releases silver ions (antimicrobial ), • Burn dressing, • May be absorbed • Sulfasalazine – (Sulfapyridine + 5-ASA) • Used in • Rheumatoid arthritis • Ulcerative colitis and
Triple Sulfa = • Sulfamethazine • Sulfadiazine • Sulfamerazine MetDiaMerza
Sulphasalazine • = • 5Amino Salicylic Acid • (Used for Ulcerative Colitis) • + • Sulphapyridine • (Used for Rheumatoid Arthritis)
Sulfasalazine Sulfapyridine 5-Amino Salicylic Acid Absorbed, Useful in RA, Produces ADR Not absorbed, Anti-inflammatory in GIT, Useful in IBD (UC, and Crohn’s disease),
Suphonamides (MOA) • Bacteria synthesize folic acid from PABA • Sulfonamide is • Structural analogue of PABA and • Inhibit Dihydrofolic Acid Synthetase • Dihydrofolic acid by Dihydrofolic acid synthetase. • Tetrahydrofolic acid by Dihydrofolic acid reductase • Tetrahydrofolic acid for synthesis of RNA, DNA
PABA antagonizes action of Sulfonamides • Pus is rich in PABA, (Purines, Pyrimidines). • Procaine local anesthetic releases PABA and reduces Sulfonamides action • Human cells • Utilize preformed Folic Acid and • Enzymes less affinity for Sulphonamides.
Sulfonamides (MOA) + PABA Dihydropteridine Sulfonamides (PABA analogues) Sulfomethoxazole (Bacterial) Sulfadiazine (Bacterial) Sulfodoxine (Malarial) Dihydropteroic acid Synthetase Static Dihydropteroic acid + Cotrimoxazole Glutamate Cidal Dihydrofolic Acid Cotrimazine Dihydrofolate Reductase Timethoprim (Bacterial) / Pyrimethamine (Malarial) Folic Acid Dihydrofolate Reductase (Mammalian) Static Tetrahydrofolic Acid RNA DNA Proteins Nucleic Bases Amino Acids
Suphonamides • Resistance is due to • Increased production of PABA • Folate synthetase affinity Less • Adoption of alternate pathway in folate metabolism • Spectrum • Primarily bacteriostatic • Both Gram positive and gram negative
Pharmacokinetics- • Orally absorbed • PPB is variable (10-95%) • Cross Placenta • Metabolized by Acetylation • By microsomal acetyl transferase • Acetylated metabolites inactive but • Produce Crystalluria
Adverse effects • Crystalluria • Dose related Tt. Fluid, Alkalizers • Fixed Drug Reaction, Hypersensitivity • Stevens-Johnson syndrome, • Photosensitization, • Hepatitis • Contact Dermatitis • Haemolysis in G-6-P-D deficiency • Kernicterus- • Premature new born, Bilirubin in brain D S P Caught Lootera Thief • Sulphur Containing Drugs (Diuretics, COX-2 inhibitors, Protease inhibitors, Antileprotics) • Dapsone • Sulfonylurea (Antidiabetic) • Protease inhibitors (Anti HIV) • Carbonic Anhydrase inhibitors,, • Celecoxib, Valdecoxib (COX-2) • Loop diuretics, • Thiazides
Fixed Drug Reactions • Fixed drug reactions are so named because they recur at the same site with each exposure • Drugs causing fixed drug eruptions: • Trimethoprim, Sulfonamides , Cotrimoxazole • Fluconazole, Ciprofloxacin, Doxycycline, Clarithromycin, NSAIDs, Phenytoin, Cetirizine, Pseudoephedrine
Fixed Drug Reactions • Usually develop within 30 minutes to 8 hours of taking the drug. • They are sometimes solitary at first, but with repeated attacks new lesions may appear and existing ones may increase in size. • Involves limbs, around mouth, eyes, genitalia and perianal areas • As healing occurs, crusting and scaling followed by brown colour at the site.
Stevens–Johnson syndrome, • A form of toxic epidermal necrolysis (TEN) • Life-threatening skin condition, • Cell death causes the epidermis to separate from the dermis. • The syndrome is thought to be a hypersensitivity complex that affects the skin and the mucous membranes. • Begins with fever, sore throat, and fatigue, and commonly misdiagnosed • Ulcers and other lesions begin to appear in the mucous membranes, almost always in the mouth and lips, but also in the genital and anal regions. • Conjunctivitis of the eyes occurs in about 30%
Characterized by confluent epidermal necrosis with minimal associated inflammation. • An idiosyncratic, delayed-hypersensitivity reaction. • Slow acetylators, Immunocompromised, and patients with brain tumors undergoing radiotherapy with concomitant antiepileptics are among those at most risk. • Patients with sulfonamide-induced toxic epidermal necrolysis have been shown to have a slow acetylator genotype that results in increased production of sulfonamide hydroxylamine . • These drug metabolites may have direct toxic effects or may act as haptens that interact with host tissues, rendering them antigenic.
Causes • Disorder of the immune system. • The immune reaction can be triggered by drugs or infections. • Genetic factors are associated with a predisposition to SJS • The cause of SJS is unknown in one-quarter to one-half of cases. • May be after viral infections, malignancies, medications. • No reliable test to establish a link between a particular drug and SJS • A leading cause sulfa drugs. • Other drugs • Allopurinol, Barbiturates,Carbazepine,Valproate, Ethosuximide, Valdecoxib, Phenytoin, Lamotrigine, • Levofloxacin, Diclofenac,, Isotretinoin, Fluconazole, , sitagliptin, , Vancomycin, Pyrimethamine, Cefixime,
Drug Interactions • Inhibit Metabolism & • Displace from protein binding site Increased Concentration of Other Drugs (Phenytoin, Tolbutamide, Warfarin, Methotrexate etc.) • Uses • Rarely used alone • Some times for chronic UTI • Topical for conjunctivitis, Burn
Cotrimoxazole • Fixed Dose Combination (FDC) of • Trimethoprim (Diaminopyridine) • + • Sulfamethoxazole (Sulfonamide) • Produce Sequential block • Combination is Cidal • (Individual component static) Preparation ratio 1:5 Ratio at site of action 1:20
Why Sulfamethoxazole? • because of similar t1/2 ( half life 10 hrs) • Why Ration of 1:5? • Trimethoprim has large volume of distribution. • Optimum synergism at ratio 1: 20 at site of action. • Why not harming human cells? • Trimethoprim is • 50,000 times active against bacterial DHFRase • Mammalian cells use preformed folic acid
Spectrum • Gram Positive • Gram negative • Drugs having Anti-folate actions • Pralatrexate • Pemetrexed • Proguanil • Pyrimethamine • Methotrexate • Trimethoprim • Resistance • Acquire DHFRase of lower affinity • Adverse effects • Same as sulfonamides • Renal toxicity • Teratogenicity • Trimethoprim, an antifolate enhance teratogenic effect • Bone marrow suppression ( in elderly) • Drug Interactions • Same as sulfonamide • Cotrimoxazole + Diuretics – Chance of thrombocytopenia
Uses of Sulphonamides and Cotrimoxazole • Faciomaxillary infections • RTI • UTI • Prostatitis • Typhoid • Bacterial diarrhea and dysentery • Pneumocystis infection in AIDS • Chancroid • Burn dressing
Cotrimoxazole • Drug of Choice • Pneumocystis pneumonia • Nocardia • Yersinia enterocolitica • As Alternative • Salmonella typhi • Shigella, E.coli • Vibrio cholerae • Brucella • Atypical mycobacterium