Download
1 / 1
10 likes | 141 Vues
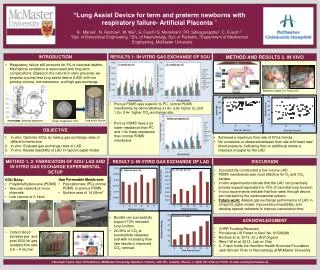
This study presents the development of a novel pump-less Lung Assist Device (LAD) aimed at supporting term and preterm newborns experiencing respiratory failure. Unlike conventional mechanical ventilation, which is linked to long-term complications, the LAD is designed to mimic natural placental gas exchange with low priming volume and resistance. In vitro results demonstrate superior oxygen and carbon dioxide exchange rates using porous polydimethylsiloxane (PDMS) membranes. Additionally, in vivo tests indicate that the LAD can effectively function in a hypoxic newborn piglet model, achieving flow rates that pose no additional stress to the cardiovascular system.

E N D
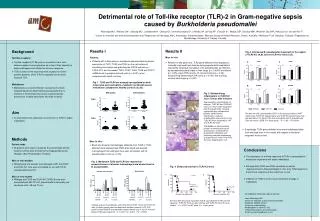
T=2 sec T=7 sec T=18 sec “Lung Assist Device for term and preterm newborns with respiratory failure- Artificial Placenta ” Manan1, N. Rochow2, W. Wu3, G. Fusch2,S. Monkman2, PR. Selvaganapthy3, C. Fusch1,2 1Dpt. of Biomedical Engineering, 2Div. of Neonatology, Dpt. of Pediatric, 3Department of Mechanical Engineering, McMaster University RESULTS 1: IN VITRO GAS EXCHANGE OF SOU METHOD AND RESULTS 3. IN VIVO INTRODUCTION • Respiratory failure still accounts for 5% of neonatal deaths. Mechanical ventilation is associated with long term complications. Based on the natural in utero placenta, we propose a pump less lung assist device (LAD) with low priming volume, low resistance, and high gas exchange. Newborn piglet 3-4 hours old • Porous PDMS was superior to PC, normal PDMS membranes by demonstrating a1.6x- 2.6x higher O2 and 1.2x- 2.4x higher CO2 exchange rate. Postnatal: artificial placenta Lung Assist Device Single Oxygenator Unit • Porous PDMS have a 2x lower resistance than PC and 1.3x lower resistance than normal PDMS membrane. OBJECTIVE In vitro: Optimize SOU, by testing gas exchange rates of different membrane. In vitro: Evaluate gas exchange rates of LAD. In vivo: Assess feasibility of LAD in hypoxic piglet model. • Achieved a maximum flow rate of 57mL/minute • No correlation is observed between flow rate and heart rate/ blood pressure, indicating that no additional stress is imposed on piglet by the LAD. membrane channel PDMS body METHOD 1, 2: FABRICATION OF SOU/ LAD AND IN VITRO GAS EXCHANGE EXPERIMENTAL SETUP DISCUSSION RESULT 2: IN VITRO GAS EXCHANGE OF LAD • Successfully constructed a low volume LAD. • PDMS membranes was most effective for O2 and CO2 transfer. • In vitro experiments indicate that the LAD can potentially provide support equivalent to 10% of neonatal lung function. • In vivo experiments indicate that flow rates through device are tolerated by the cardiovascular system. • Future work:Assess gas exchange performance of LAD in a hypoxic piglet model, improve biocompatibility, and develop special catheters to improve cannulation time. • SOU Body: • Polydimethylsiloxane (PDMS) • Vascular network of micro channels • Low volume of 0.14mL • Gas Permeable Membrane: • Polycarbonate (PC),normal PDMS, or porous PDMS • Surface area of 14.08cm2 • Bundle can successfully support 10% neonatal lung function. • 20-30% of CO2 is successfully released, and with increasing flow rate results in improved CO2 removal. ACKNOWLEDGMENT • CHRP Funding Received • Provisional US Patent is filed, No. 61526288 • Rochowet al, 2013. Int J Artif Organs • Wen-I-W et al, 2013. Lab on Chip • C. Fusch holds the Hamilton Health Sciences Foundation Jack Sinclair Chair in Neonatology at McMaster University • Collect blood samples pre- and post SOU for gas analysis flow rate: 0.5 – 4 mL/min Christoph Fusch, Dpt. Of Pediatrics, McMaster University, Hamilton, Ontario, L8S 4K1, Canada, Phone: +1 (905) 521 2100 ext 75721, E-mail: fusch@mcmaster.ca