Download
1 / 54
560 likes | 861 Vues
Board Review: Gastroenterology. ANSWERS. Board Review: Gastroenterology 1.

E N D
Board Review:Gastroenterology ANSWERS
Board Review: Gastroenterology 1 • A 2.4-kg term infant who has the clinical features of Down syndrome has bile-stained emesis following a cow milk-based formula feeding 4 hours after birth. Physical examination reveals abdominal distension. A “double bubble” is seen on the abdominal flat plate radiograph. No air is present elsewhere in the abdomen.Of the following, the BEST initial step in management of this infant is: A. administration of intravenous antibiotic B. contrast enema C. emergent surgical decompression D. nasogastric tube placement E. soy milk formula feeding 2005/question 3
Board Review: Gastroenterology The double bubble sign is the radiologic hallmark of duodenal atresia, which often is associated with Down syndrome (trisomy 21). The presence of bile-stained emesis reported for the infant described in the vignette is an additional indication of an upper gastrointestinal tract obstruction and constitutes a neonatal emergency. Initial management includes making the patient non per os (NPO), providing intermittent gastric suction with a large-bore nasogastric tube, ensuring both fluid and electrolyte balance, and consulting a pediatric surgeon. Surgical exploration, decompression, and repair would follow this initial management.A contrast enema would be appropriate to evaluate a lower gastrointestinal tract obstruction, typically presenting after 24 hours with abdominal distension and delayed or absent passage of stool. Cow milk protein enterocolitis or lactose intolerance occurring after days of feeding may be manifested by bloody stools or emesis (not bile-stained), eliminating the need for changing the feeding to soy milk formula. Antibiotics are not the best initial step in the management of an infant who has a bowel obstruction.
Board Review: Gastroenterology 2 • A 15-year-old girl presents with her third episode of severe epigastric pain in the past 8 months. In between episodes, she is completely healthy. In each of her prior episodes, amylase and lipase concentrations both were elevated (>500 U/L), but returned to normal within 96 hours. The girl states that she does not consume alcohol and takes no medications. A brother has been hospitalized with similar symptoms. On physical examination, the girl appears well nourished but uncomfortable and is experiencing moderate epigastric tenderness. Complete blood count, transaminases, and bilirubin results are normal; the amylase level is 700 U/L and lipase level is 1,100 U/L. You admit the girl to the hospital for hydration and pain control. Abdominal ultrasonography shows no gallstones, and the common bile duct is not dilated. The pancreas is slightly enlarged, but there is no pseudocyst.Of the following, the MOST appropriate next test to identify the cause of this girl’s illness is: A. esophagogastroduodenoscopy B. genetic testing for Johanson-Blizzard syndrome C. mumps antibody titer D. sphincter of Oddi manometry E. sweat test for cystic fibrosis 2005/question 18
Board Review: Gastroenterology Most children who present with pancreatitis have a readily identifiable cause, including trauma, biliary tract disease, medication, or vasculitis. However, a subset of patients present with recurrent or chronic pancreatitis without an identifiable cause. It is essential to evaluate these patients for genetic and anatomic causes of pancreatitis, including cystic fibrosis (CF). CF is one of the most common hereditary causes of recurrent pancreatitis. Patients who have CF and recurrent pancreatitis typically present during adolescence and may not have any obvious signs of pancreatic insufficiency or chronic lung disease, such as the girl described in the vignette. Accordingly, this girl should undergo a sweat test for CF. Another subset of patients who have recurrent pancreatitis have mutations in the cystic fibrosis transmembrane regulator (CFTR) gene, but they do not have the CF phenotype.Other genetic mutations that can cause chronic or recurrent pancreatitis include alterations in the cationic trypsinogen gene or mutations in SPINK-1. Anatomic factors that may predispose to recurrent pancreatitis include pancreas divisum and long common channel. Pancreas divisum is a congenital variant occurring in 2% of the normal population. In a subset of these patients, ineffective ductal drainage from the main duct may predispose to pancreatic obstruction. In long common channel, biliary and pancreatic juices may mix, thus activating pancreatic enzymes within the pancreas.Although esophagogastroduodenoscopy can identify ulcers or other causes of epigastric pain, it cannot identify anatomic abnormalities within the pancreatic ducts. To identify the abnormalities discussed previously, endoscopic retrograde cholaniopancreatography (ERCP) is necessary. Johannson-Blizzard syndrome is an autosomal recessive condition causing facial dysmorphism and pancreatic insufficiency. It is not a cause of recurrent pancreatitis, and there is no genetic test available for this condition. Pancreatitis can occur as a result of mumps infection, but this should not trigger recurrences. Sphincter of Oddi manometry is a sophisticated test that uses ERCP and manometric catheters to measure sphincter pressure. The role of this test in the evaluation of children who have recurrent pancreatitis has yet to be established.
Board Review: Gastroenterology 3 • A 3,200-g term male infant presents for his 1-week evaluation. The pregnancy and delivery were uneventful. His parents state that the baby has been difficult to arouse, is feeding poorly, and has been vomiting. On physical examination, the infant weighs 2,800 g, is lethargic and jaundiced, and has a palpable liver 3 cm below the right costal margin. An evaluation for sepsis has been performed and antibiotic therapy initiated. Additional laboratory results include: total bilirubin, 18 mg/dL (307.8 mcmol/L); direct bilirubin, 6 mg/dL (102.6 mcmol/L); alanine aminotransferase, 104 U/L; aspartate aminotransferase, 150 U/L; and positive urine dipstick for protein and reducing substances.Of the following, the test that would be MOST helpful in the diagnosis of this patient is A. Coombs test and maternal anti-Rh titer B. examination of a blood smear for red cell morphology C. serum amino acids and urine organic acids D. serum galactose-1-phosphate uridyltransferase level E. serum hepatitis B surface antigen 2005/question 37
Board Review: Gastroenterology Direct or conjugated hyperbilirubinemia in the neonatal period may result from intrinsic liver disease or a congenital hepatobiliary obstruction. In these cases, conjugated bilirubin levels increase rapidly during the first few postnatal weeks to greater than 2 mg/dL (34.2 mcmol/L) and remain elevated. Underlying causes include bacterial or viral sepsis, nonspecific neonatal hepatitis, galactosemia and other metabolic disorders (tyrosinemia, fructosemia, Niemann-Pick disease, Gaucher disease, glycogenosis Type IV, cystic fibrosis), severe hemolysis (with inspissation of bile, which may be seen in Rh disease), biliary atresia, extrahepatic biliary obstruction, alpha-1-antitrypsin deficiency, isolated defects in hepatic bilirubin transport, and neonatal hemosiderosis. A prompt investigation should be undertaken to determine the cause of the conjugated hyperbilirubinemia because some of the causative conditions may be serious and life-threatening and have significant implications for the child’s health and future development.The symptoms exhibited by the infant described in the vignette, coupled with their time of onset and the presence of reducing substances in the urine, suggest the diagnosis of galactosemia. Therefore, measurement of the serum galactose-1-phosphate uridyltransferase level would be the most helpful. Obtaining a Coombs test and maternal anti-Rh titer, serum amino acids and urine organic acids measurements, and a peripheral blood smear is appropriate for the evaluation of an infant who has unconjugated hyperbilirubinemia. Hepatitis B virus infection may cause conjugated hyperbilirubinemia, but the patient's age and clinical presentation are not consistent with neonatal hepatitis B infection.
Board Review: Gastroenterology 4 • A 13-year-old girl reports, “I’m just not feeling like myself.” In the past month, she has noted progressive fatigue, to the point of falling asleep in class. Her mother has noticed that the girl seems more prone to nosebleeds, and her skin color has changed. Physical examination demonstrates an alert, slightly jaundiced child who has mild scleral icterus and two small bruises on each of her forearms. Her throat appears normal and without exudates. There is no adenopathy. Her liver span is 11 cm (4 cm below the costal margin), and a spleen tip is palpable. Laboratory studies demonstrate an aspartate aminotransferase of 740 U/L, alanine aminotransferase of 1,390 U/L, total bilirubin of 5 mg/dL (85.5 mcmol/L), direct bilirubin of 2 mg/dL (34.2 mcmol/L), prothrombin time of 20 sec, albumin of 2.0 g/dL (20 g/L), and total protein of 9.0 g/dL (90 g/L). Findings on the complete blood count are unremarkable.Of the following, the diagnosis that is MOST consistent with the findings is: A. alpha-1-antitrypsin deficiency B. autoimmune hepatitis C. hepatitis C D. infectious mononucleosis E. Wilson disease 2005/question 47
Board Review: Gastroenterology Five principal mechanisms result in hepatomegaly: passive congestion of the liver from heart failure or hepatic venous obstruction, inflammation (hepatitis), infiltration by tumor, a storage disorder causing engorgement of hepatocytes, and hepatic cirrhosis. The first three (obstruction, inflammation, and tumor) may cause an enlarged, tender liver. In patients who have storage disorders (glycogen storage disease, mucopolysaccharidosis), the liver typically is nontender. Cirrhosis generally presents with a firm, fibrotic liver and signs of portal hypertension (splenomegaly).The adolescent girl described in the vignette presents with hepatomegaly, markedly elevated transaminases, jaundice, coagulopathy, hypoalbuminemia, and an elevated total protein concentration. The elevated total protein in the context of hypoalbuminemia suggests an elevated globulin fraction. This finding is strongly suggestive of autoimmune hepatitis, in which autoantibodies are manufactured that mediate damage to the liver parenchyma. There are two types of autoimmune hepatitis. Type 1 is characterized by the presence of anti-smooth muscle antibodies and occurs most commonly in adolescent and young adult females. Type 2 autoimmune hepatitis is characterized by the presence of anti-liver-kidney microsomal antibodies and may occur in young children. Autoimmune hepatitis may occur following the administration of medications such as minocycline. The diagnosis is established by liver biopsy, which demonstrates a portal infiltrate of lymphocytes and plasma cells. However, for the patient in the vignette, careful attention is needed to correct her coagulopathy before considering a closed biopsy. It is important to recognize this condition because the administration of corticosteroids and azathioprine may be lifesaving.Although alpha-1-antitrypsin deficiency, hepatitis C, and infectious mononucleosis may present with hepatic inflammation and hepatomegaly, the severity of the presentation described in the vignette makes these diseases less likely. Wilson disease can present in adolescence with severe liver disease and coagulopathy and should be excluded in this patient, but the elevated total protein (hypergammaglobulinemia) is more consistent with autoimmune hepatitis.
Board Review: Gastroenterology 5 • You are evaluating a 2-week-old infant in the clinic for jaundice. He had mild jaundice in the first 5 postpartum days that subsided at the end of the first week. He breastfeeds well and passes stool and urine numerous times each day. His weight is 7 oz (200 g) greater than his birthweight. He is alert and active on physical examination, with normal neuromotor tone and no hepatosplenomegaly. The total serum bilirubin concentration is 19 mg/dL (325 mcmol/L), and the conjugated fraction is 1.0 mg/dL (17.1 mcmol/L).Of the following, the BEST management for this infant is to A. admit for phototherapy B breastfeed more frequently C. cease breastfeeding and begin cow milk-based formula feeding D. interrupt breastfeeding for 48 hours E. provide the baby with supplemental glucose water 2005/question 111
Board Review: Gastroenterology Jaundice is a frequent neonatal condition, affecting more than 30% of newborns. Physiologic jaundice is, in most instances, benign and resolves in the first 3 to 7 postnatal days. When hyperbilirubinemia occurs early (<24 hours of age), rises quickly or to a potentially dangerous level, is prolonged, or recurs, as described for the infant in the vignette, it requires investigation. In evaluating jaundice, the total and the conjugated fraction of bilirubin must be determined. Maternal and infant blood type(s), Rh status, and indices of neonatal hemolysis (eg, direct Coombs test) would be assessed as indicated.Jaundice also may be associated with breastfeeding, conferring a higher peak total serum bilirubin (TSB) concentration and requiring a longer resolution compared with jaundice among infants receiving cow milk-based formula or protein hydrolysate formula. In such cases, more frequent breastfeeding would be acceptable, but in breast-milk jaundice, breastfeeding needs to be interrupted.The patient described has breast-milk jaundice, seen in only a small number of infants (<2%). This phenomenon occurs in the second postnatal week and is believed to be due to either an exaggeration of the enterohepatic recirculation or the presence of beta-glucuronidase or another substance in the milk.It is diagnosed after excluding other potential causes of elevated indirect hyperbilirubinemia.It responds very well to an interruption of human milk feedings for 24 to 48 hours, resulting in a rapid decline in the TSB and avoiding the necessity of other interventions such as phototherapy or exchange transfusion. Although this brief interruption is necessary, there is no reason to cease breastfeeding absolutely; it should be resumed after 24 to 48 hours of cow milk- or soy-based formula. The provision of glucose water is neither beneficial nor sufficient to address the infant's nutritional needs.
Board Review: Gastroenterology 6 • A 12-year-old boy presents to the emergency department because of progressive, intermittent, crampy abdominal pain and bilious vomiting for the past 12 hours. He has had two watery bowel movements in the last 36 hours and has not voided in 6 hours. Two weeks ago, he had a laparotomy and ileal resection for Crohn disease.Of the following, the clinical finding that MOST favors a diagnosis of postoperative small bowel obstruction rather than ileus is: A. abdominal distension B. decreased urine output C. hyperactive bowel sounds D. paucity of stool on rectal examination E. tachycardia 2005/question 124
Board Review: Gastroenterology The patient described in the vignette presents with crampy abdominal pain, vomiting, and possibly decreased urine output. He has a recent history of abdominal surgery. This nonspecific presentation could be caused by gastroenteritis, but the recent history of surgery raises the possibility of both postoperative small bowel obstruction (SBO; mechanical obstruction) and paralytic ileus. The occurrence of symptoms 2 weeks after the surgery is more consistent with bowel obstruction than ileus.Both ileus and SBO may be associated with symptoms of abdominal pain, dehydration, and vomiting. Third spacing of fluid into the abdomen may result in abdominal distension, intravascular volume depletion, tachycardia, and decreased urine output. A physical examination typically reveals an uncomfortable patient who has a distended abdomen. For a patient who is unable to provide a history, the abdomen should be examined for surgical scars. Postoperative ileus is characterized by a paucity or absence of bowel sounds. In contrast, SBO may feature hyperactive or high-pitched bowel sounds. Absence of stool in the rectum does not imply obstruction because a patient may pass stool distal to an obstructed bowel.The differential diagnosis of a mechanical SBO is broad and includes postsurgical adhesions, acute appendicitis, incarcerated inguinal hernia, intussusception, malrotation with volvulus, sigmoid volvulus, and Meckel diverticulum. For a patient who has a prior history of abdominal surgery, adhesions are by far the most common cause of SBO. The diagnosis usually can be established easily with flat and upright abdominal radiographs, which may demonstrate dilated small bowel with air fluid levels. If the bowel is filled completely with fluid, however, pathognomonic findings of SBO on plain film may be difficult to identify. In these cases, computed tomography may provide useful information or laparotomy may be necessary. Contrast examinations may be useful in partial obstructions, but are contraindicated in high-grade obstructions.The management of a bowel obstruction includes decompression with a nasogastric tube, correction of dehydration with a normal saline (0.9% NaCl) bolus, and administration of maintenance and replacement fluid (usually 5% dextrose with half normal saline [D5 + 0.45% NaCl]). Electrolyte levels should be measured at initial evaluation and followed carefully. With high obstructions, hypochloremic metabolic alkalosis may occur. Severe pain in a patient who has a suspected bowel obstruction, acidosis, or hyperkalemia suggest bowel ischemia or necrosis and requires prompt surgical intervention.
Board Review: Gastroenterology 7 • A 2-year-old girl has a history of biliary atresia treated with a Kasai procedure at 3 months of age. She presents to the emergency department because she vomited “a cupful” of blood that morning. She is pale and quiet. You examine the patient, administer a normal saline bolus, and send blood for diagnostic studies.Of the following, the finding that suggests bleeding from esophageal varices rather than from gastritis or peptic ulcer disease is a: A. bilirubin of 8 mg/dL (136.8 mcmol/L) B. diagnosis of vitamin D-deficient rickets C. history of ibuprofen administration 24 hours ago D. prothrombin time of 19 sec E. spleen extending 5 cm below the costal margin 2005/question 146
Board Review: Gastroenterology The differential diagnosis of hematemesis in a child is fairly limited and includes erosive esophagitis, gastritis, peptic ulcer disease, arteriovenous malformations, Dieulafoy lesion (a rare vascular anomaly of the stomach associated with an overlying mucosal defect), and bleeding from esophageal or gastric varices. Esophageal variceal bleeding almost always is caused by portal hypertension, although occasionally it can be caused by shunting from complex cardiac and vascular malformations. Splenomegaly usually is present in patients who have portal hypertension and should raise the suspicion of variceal bleeding, especially if a patient has a history of significant liver disease. In portal hypertension, elevated pressures in the portal venous system result in increased shunting of venous blood through collaterals in the azygous system, with resultant splenic enlargement and dilation of esophageal and hemorrhoidal veins. These veins initially dilate to accommodate the increased pressure, but can rupture if the wall tension on the vein becomes too great.Portal hypertension may be subdivided into three groups: "prehepatic," due to a thrombosis or occlusion of the portal vein; "intrahepatic," due to hepatic cirrhosis; and "posthepatic," due to a thrombosis in the hepatic vein, inferior vena cava, or right atrium. Portal vein thrombosis often is called "cavernous transformation of the portal vein" because of the network of collaterals that develops around the liver. Hepatic venous thrombosis is referred to as Budd-Chiari syndrome. Most cases of biliary atresia are at risk for hepatic cirrhosis even with a functioning Kasai procedure, as in this patient's case.Therapy of portal hypertension includes: pharmacologic management with propranolol to lower portal venous pressure, endoscopic sclerotherapy and band ligation to ablate varices that have bled, and creation of a surgical shunt between the systemic and portal venous systems (eg, portocaval or splenorenal) to decompress the portal system. The finding of splenomegaly in the girl described in the vignette is the only feature that specifically suggests portal hypertension. Hyperbilirubinemia, coagulopathy, and vitamin D deficiency all suggest hepatocellular injury and cholestasis, but they do not specifically suggest portal hypertension. The history of ibuprofen intake raises the suspicion of gastritis or ulcers from nonsteroidal anti-inflammatory medications.
Board Review: Gastroenterology 8 • A 15-year-old girl presents with a 3-week history of fatigue, a 2-week history of temperature to 100.4°F (38°C), and a 1-week history of jaundice. She admits to both unprotected intercourse and intravenous drug use. On physical examination, she has an enlarged liver, with a span of 9 cm (4 cm below the right costal margin). Laboratory studies demonstrate an aspartate aminotransferase level of 460 U/L and an alanine aminotransferase level of 760 U/L.In a patient of this age, the viral infection that is associated with the HIGHEST risk for the development of chronic hepatitis and cirrhosis is: A. Epstein-Barr B. hepatitis A C. hepatitis B D. hepatitis C E. hepatitis E 2005/question 152
Board Review: Gastroenterology The girl described in the vignette presents with malaise, fever, and jaundice and has risk factors for hepatitis B, hepatitis C, and human immunodeficiency virus infection. The absence of signs of chronic liver disease (ascites, splenomegaly, telangiectasias) suggests an acute hepatitis. If the patient has normal coagulation study results, normal ammonia levels, and normal findings on neurologic examination, liver failure is not currently present.The initial serologic evaluation should include hepatitis A antibody; hepatitis B surface antigen, core antibody, and surface antibody; and hepatitis C antibody. Hepatitis A may be spread by infected food or close personal contact and are mild and self-limited. Hepatitis A can cause fulminant liver failure in 1% of adults and rarely in children.. Hepatitis B is a DNA-containing virus and transmission is through close personal contact, needle sharing, unprotected intercourse, and from mother to child. Adults infected with hepatitis B typically have acute hepatitis symptoms only; more than 80% successfully clear surface antigen and develop surface antibody.Hepatitis C virus is an RNA virus with transmission through needles, blood, or close personal contact in a manner similar to hepatitis B. In contrast to the high vertical transmission rate of hepatitis B, the transmission rate from mother to child of hepatitis C is approximately 5%. The symptoms in the acute phase of infection are very mild and may include anorexia, malaise, and abdominal pain; most patients are anicteric. Unfortunately, patients infected with hepatitis C have a 50% to 80% chance of developing chronic hepatitis and a 10% to 20% chance of developing cirrhosis. The persistence of elevated aminotransferase concentrations after 6 months in a patient who has a documented hepatitis B or C infection suggests ongoing chronic liver disease and warrants referral for consideration of antiviral therapy.
Board Review: Gastroenterology 9 • A 17-year-old boy is brought in by his parents because they claim his eyes “look yellow” in the morning. He feels well and is active in sports. His past medical history is unremarkable. The boy’s father had acute hepatitis B 12 years ago. The boy has minimal scleral icterus, no tattoos or body piercing, normal heart sounds, no jugular venous distension, and no hepatomegaly or splenomegaly. Laboratory studies demonstrate a total bilirubin of 2.3 mg/dL (39.3 mcmol/L) and direct fraction of 0.1 mg/dL (1.71 mcmol/L). Aspartate aminotransferase and alanine aminotransferase both measure 20 U/L, alkaline phosphatase is 200 U/L, and gamma glutamyl transpeptidase is 40 U/L. Hepatitis B surface antigen is negative.Of the following,the MOST likely cause of this boy’s jaundice is: A. autoimmune hepatitis B. Crigler-Najjar syndrome type 2 C. Gilbert syndrome D. hepatitis C E. primary sclerosing cholangitis 2005/question 153
Board Review: Gastroenterology The patient described in the vignette appears healthy, but he has a mild unconjugated hyperbilirubinemia. Physical examination results and measurements of transaminases, alkaline phosphatase, and gamma-glutamyl transpeptidase are normal. The findings strongly suggest Gilbert syndrome, a heterogeneous group of genetic mutations of the UDPGT enzyme that result in mildly decreased conjugation of bilirubin. The genetic decrease in UDPGT function is associated with an increased number of thiamine-adenine repeats in the promoter region (TATA box) of the gene. Gilbert syndrome is estimated to occur in 1% to 3% of the general population and is believed to have no significant health sequelae or complications. No therapy is necessary, and management consists of education and reassurance.Generally, Gilbert syndrome can be diagnosed on the basis of history and physical examination. Jaundice typically is more pronounced in the morning and can be exacerbated by an overnight fast. If there is a typical history, unconjugated bilirubin ranges from 1 to 4 mg/dL (17.1 to 68.4 mcmol/L), and other liver test results are normal, no further evaluation is necessary. If more formal diagnostic testing is desired, high-performance liquid chromatography demonstrates decreased bilirubin monoglucuronides. Genetic testing also has been performed in some patients to evaluate for promoter mutations.Crigler-Najjar syndromes types 1 and 2 are more severe, autosomal recessive forms of nonhemolytic jaundice. Type 1 is the most severe form and is characterized by virtual absence of UDPGT function. Children present in the first postnatal month with severe indirect hyperbilirubinemia (bilirubin levels >20 mg/dL [342 mcmol/L]) and are at risk of kernicterus. Treatment involves life-long phototherapy and, when appropriate, liver transplantation. Crigler-Najjar type 2 (Arias syndrome) also results in significant jaundice, but bilirubin levels are somewhat lower (10 to 25 mg/dL [171 to 427.5 mcmol/L]) and can be lowered by phenobarbital therapy. Autoimmune hepatitis is characterized by transaminase elevation and hypergammaglobulinemia. Hepatitis C is a viral infection that most commonly causes transaminase elevation without jaundice. Primary sclerosing cholangitis (PSC) is a rare condition causing bile duct scarring, jaundice, and cholestasis. In PSC, the hyperbilirubinemia is direct, and GGTP and transaminases usually are elevated.
In Gilbert's Syndrome there may be a deficiency of either ligandin, (1) a protein which binds bilirubin and may assist in its transport to the endoplasmic reticulum for conjugation, or in UDPglucuronyl transferases. Deficiency in either one would result in defective bilirubin conjugation (2) with glucuronic acid by the endoplasmic reticulum. The net result would be a decreased conjugation of bilirubin and impaired excretion of bilirubin into the bile.
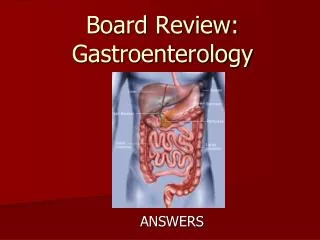
Board Review: Gastroenterology 10 • A 10-year-old boy presents with the acute onset of abdominal pain that was followed shortly thereafter by vomiting. The pain is described as periumbilical. There is no history of trauma. He has had no fever, sore throat, headache, dysuria, or diarrhea. His mother describes the emesis as “green.”On physical examination, the child is in obvious distress. Other than mild tachycardia, his vital signs are within normal limits. His abdomen is diffusely tender, with localization to the periumbilical area. He also complains of increased abdominal pain when his heel is struck by the examiner’s hand. Rectal examination reveals no evidence of occult blood.Of the following, the MOST likely cause of this child’s abdominal pain is: A. acute pancreatitis B. appendicitis C. intussusception D. pyelonephritis E. small bowel obstruction 2005/question 173
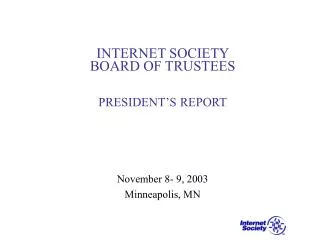
Board Review: Gastroenterology Acute appendicitis is one of the most common abdominal surgical conditions seen by pediatricians. The initial periumbilical location of the pain with subsequent localization to the right lower quadrant is most consistent with acute appendicitis. During the early evolution of appendicitis, the inflammation causes referred pain to the periumbilical region, as described for the boy in the vignette. As the inflammation becomes more intense, somatic nerve fibers on the abdominal wall and surrounding structures are stimulated, resulting in the more localized pain at McBurney point, which is located one third of the distance from the iliac crest to the umbilicus.The pain of pancreatitis can occur throughout the abdomen, but characteristically it is localized in the epigastrium or right upper quadrant, with radiation to the back. Intussusception causes short periods of severe pain alternating with longer periods without pain as successive peristaltic waves arrive at the site of the obstruction. Pyelonephritis may cause abdominal pain, but most frequently it causes flank tenderness with associated fever and dysuria. Small bowel obstruction can mimic all the symptoms of appendicitis, but the tenderness tends to be more diffuse. In addition, this diagnosis is much less likely in a child who has had no prior abdominal surgery.
Acute appendicitis. Axial CT scans obtained with intravenous contrast show a minimally distended appendix with an enhancing wall (arrow). Stranding is seen in the periappendiceal fat. These findings are pathognomonic for acute appendicitis.
Board Review: Gastroenterology 11 • You are seeing an 8-year-old boy for the first time for a health supervision visit. The family emigrated 2 years ago from China. The mother has chronic hepatitis B, but her son’s hepatitis status never has been evaluated, and the mother does not know whether the boy has been immunized. She wonders if he is at risk for chronic hepatitis B and its complications.Of the following, the serologic profile that is MOST suggestive of chronic hepatitis B resulting from perinatal infection is: A. Hepatitis B surface antigen: negative; Hepatitis B core antibody: negative; Hepatitis B e antigen: negative; Hepatitis B surface antibody: negative B. Hepatitis B surface antigen: negative; Hepatitis B core antibody: negative; Hepatitis B e antigen: negative; Hepatitis B surface antibody: positive C. Hepatitis B surface antigen: positive; Hepatitis B core antibody: positive; Hepatitis B e antigen: negative; Hepatitis B surface antibody: positive D. Hepatitis B surface antigen: negative; Hepatitis B core antibody: negative; Hepatitis B e antigen: positive; Hepatitis B surface antibody: negative E. Hepatitis B surface antigen: positive; Hepatitis B core antibody: positive; Hepatitis B e antigen: negative; Hepatitis B surface antibody: negative 2005/question 190
Board Review: Gastroenterology Transmission is primarily through vertical transmission from mother to infant or through exposure to blood or semen. In approximately 30% to 40% of cases, no obvious risk factor can be identified. Approximately 90% of older children and adults clear an acute infection of hepatitis B. In contrast, more than 80% of infants contracting hepatitis B from their mothers become chronic carriers if not immunized with hepatitis B vaccine appropriately and given hepatitis B immune globulin at birth.In acute infection, hepatitis B surface antigen (HepBsAg) typically appears in the serum of an infected patient after an incubation period of 45 to 160 days. Concurrently, hepatitis B e antigen(HepBeAg) also may be elevated; the e antigen implies a high level of viral load and infectivity. At this time, the symptomatic patient experiences malaise, fatigue, nausea, and jaundice, and transaminases are elevated. The symptomatic period lasts approximately 4 weeks. In a patient who resolves the infection, the HepBsAg and HepBeAg become negative after 6 months, and antibody to hepatitis B surface antigen (anti-HBs) appears.In contrast, in a patient who has chronic hepatitis B infection, HepBsAg (and sometimes HepBeAg) persist, transaminases may stay elevated, and anti-HBs fails to form. Patients who have chronic hepatitis B are at increased risk for cirrhosis and hepatocellular carcinoma.Antibody to hepatitis B core (anti-HepBc) is formed after exposure to the virus. Although these antibodies do not protect against viral infection, they are useful as serologic markers to determine if a patient has been exposed to hepatitis B. Immunization protects against hepatitis B because it generates antibodies to surface antigen. Patients who have been immunized are anti-HBs-positive, but have no core antibody (anti-HepBc-negative). In contrast, patients who have past infection have both anti-HBs and anti-HepBc.The serologic profile in patient "E" has evidence of both surface antigen and core antibody, with no surface antibody. This suggests chronic infection.Patient "A" has negative HepBsAg, anti-HepBc, HepBeAg, and anti-HBs and has never been exposed to, or immunized against, hepatitis B.Patient "B," who has negative HepBsAg, anti-HepBc, and HepBeAg in conjunction with positive anti-HBs, has been immunized, but has no evidence of past or current HBV infection. The other two profiles (Patient "C" and "D") most likely represent laboratory errors. A patient cannot have both HepBsAg and anti-HBs. Similarly, HepBeAg cannot be present in the absence of HepBsAg.
Board Review: Gastroenterology 12 • You are spending 2 months at a locum tenens in Greenland, caring for the native population of Eskimos. A family brings in a 1-year-old infant who has failure to thrive, diarrhea, and abdominal distension. The baby has been breastfed since birth. The growth chart reveals that the baby grew normally until 6 months of age. Between 6 and 12 months of age, the weight decreased from the 50th to the 5th percentile, while the height remained at the 50th percentile. Solid foods were introduced at 6 months of age, with breastfeeding continuing. Dietary history shows that the caloric intake is appropriate for age. On physical examination, the alert but thin infant has a distended abdomen and a perianal rash. The stool is watery and foul-smelling and has a pH of 3. No parasites are identified in the stool. Fecal fat and fecal alpha-1-antitrypsin measurements are both within normal limits.Of the following, the MOST likely diagnosis is: A. congenital lactose intolerance B. cystic fibrosis C. hereditary fructose intolerance D. intestinal lymphangiectasia E. sucrase-isomaltase deficiency 2005/question 192
Board Review: Gastroenterology The infant described in the vignette presents with a falloff in weight percentiles, abdominal distension, a perianal rash, and watery stool. The normal levels of stool fat and alpha-1-antitrypsin suggest that the baby does not have fat or protein malabsorption, as seen in cystic fibrosis. The acidic stool pH suggests bacterial fermentation of carbohydrates and carbohydrate malabsorption.Ingested complex carbohydrates (eg, starch) are broken down by pancreatic amylase to di- and trisaccharides, which are broken down further by sucrase-isomaltase and glucoamylase at the level of the intestinal brush border. Lactose (milk sugar), a disaccharide composed of galactose and glucose, is broken down to its component monosaccharides by lactase. Sucrose (table sugar) is a disaccharide composed of glucose and fructose that is broken down to its component monosaccharides by the enzyme sucrase-isomaltase. Monosaccharides then may be transported across the enterocyte by specific transport molecules.Carbohydrate malabsorption may be either primary or secondary. Secondary malabsorption of carbohydrates occurs during and after an illness that damages the bowel (eg, rotavirus infection, giardiasis, or celiac disease). Lactase is located on the tips of intestinal villi and is the enzyme most susceptible to villous damage. Thus, in rotaviral infection, villous damage results in clinically significant lactose intolerance in 20% to 30% of infants. In contrast, the most common congenital disaccharidase deficiency is sucrase-isomaltase deficiency, an autosomal recessive condition. The prevalence in most populations is less than 1:1,000, but in Canadian Indians and Greenland Eskimos, the prevalence is as high as 5%. Infants usually present after 6 months of age, when starch- or sucrose-containing foods are introduced into the diet. The diagnosis is established by intestinal biopsy and assay for disaccharidase activity. Treatment involves a combination of dietary restriction of sugars and starches and supplementation with exogenous sucrase enzyme.Congenital lactose intolerance is extraordinarily rare and appears in early infancy, after the institution of milk feedings. Infants who present as the one in the vignette should be screened for cystic fibrosis, but there is no evidence of fat malabsorption or pulmonary disease in the described baby. Similarly, intestinal lymphangiectasia presents with diarrhea, edema, and evidence of fat malabsorption.Hereditary fructose intolerance (fructose-1-phosphate aldolase deficiency) presents not only with diarrhea, but with severe liver injury, hepatomegaly, coagulopathy, and renal Fanconi syndrome.
Board Review: Gastroenterology 13 • A 3-year-old girl is brought to the emergency department with a history of blood in her stool. In the past 12 hours, she has had three large, mushy bowel movements that the parents say had about 2 tablespoons of blood mixed in with each stool. She has not vomited. She has been afebrile and does not appear uncomfortable when passing the stool. On physical examination, the frightened but active toddler is in no distress. Her abdomen is soft, and rectal examination demonstrates dark red blood. The hematocrit is 25% (0.25), platelet count is 350 x 103/mcL (350 x 109/L), white blood cell count is 9 x 103/mcL (9 x 109/L), prothrombin time is 12.5 sec, and partial thromboplastin time is 25 sec.Of the following, the next MOST appropriate diagnostic procedure is: A. abdominal computed tomography B. colonoscopy C. exploratory laparotomy D. nasogastric tube placement E. 99mTc-pertechnetate scan 2005/question 221
Board Review: Gastroenterology The differential diagnosis of hematochezia in a toddler can be subdivided into conditions causing painful or painless rectal bleeding. Painful rectal bleeding suggests bowel inflammation (especially colitis) or bowel ischemia. The pain associated with colitis usually accompanies the bowel movement and is relieved by the passage of stool; the most common causes of colitis are infection (eg, Salmonella, Shigella, Yersinia, and Campylobacter sp; Escherichia coli; Clostridium difficile; and amoeba) and inflammatory bowel disease. In contrast, bowel pain associated with ischemia is crampy, severe, and independent of the bowel movement. Common causes of ischemic pain include vasculitides (eg, Henoch-Schönlein purpura) and intussuception.Although hemorrhoids and anal fissures can cause rectal bleeding, such bleeding usually is trivial.Large-volume painless rectal bleeding, as reported for the child in the vignette, suggests a specific, localizable lesion. The most common causes of such painless rectal bleeding in children are Meckel diverticulum and colonic juvenile polyps. Among the less common causes are hemangiomas and venous malformations (such as those seen in blue rubber bleb nevus syndrome). Meckel diverticulum is a persistent remnant of the omphalomesenteric duct that is identified in 2% of the population. A typical Meckel diverticulum is approximately 5 cm (2 in) long and located on the antimesenteric border of the ileum, approximately 60 cm from the ileocecal valve. The three most common complications of symptomatic Meckel diverticulum are gastrointestinal bleeding, bowel obstruction from infection or incarceration, and infection (Meckel diverticulitis).A bleeding Meckel diverticulum occurs when the diverticulum contains ectopic gastric mucosa. The ectopic mucosa may secrete acid, which causes ulceration of the adjacent tissue and bleeding. A child who has Meckel diverticulum typically presents acutely, with large-volume (>30 mL) rectal bleeding that may require transfusion. In contrast, colonic polyps present more commonly with a history of intermittent small-volume (<5 mL) rectal bleeding. If a Meckel diverticulum is suspected, a 99mTc-pertechnetate scan identifies the lesion approximately 80% of the time. This uptake can be enhanced with agents like cimetidine, glucagon, and gastrin administered prior to the study. Management of the Meckel diverticulum involves hemodynamic stabilization of the patient, followed by surgical resection.A patient who has rectal bleeding and a negative scan should undergo colonoscopy to evaluate for colitis or polyps. If the colonoscopy is negative, the patient continues to bleed, and Meckel diverticulum still is suspected strongly, consideration should be given to other imaging modalities (eg, computed tomography) or even laparotomy. Nasogastric tube placement is useful in the diagnosis and treatment of upper gastrointestinal bleeding, but usually is not indicated in the management of a patient who has hematochezia.
Meckel’s Diverticulum • The “rule of 2” with Meckel’s diverticulum: • 2% occurrence • two types of lining (stomach and pancreas • within 2 ft of the small/large intestinal junction • approximately 2 inches in length • symptomatic by 2 years of age
Board Review: Gastroenterology 14 • A 2-month-old girl presents to the emergency department with a 1-month history of irritability and nonbilious vomiting. The vomiting has increased gradually, and the child now appears mildly dehydrated. Hematocrit is 35%, serum sodium level is 130 mEq/L, chloride is 93 mEq/L, bicarbonate is 27 mEq/L, glucose is 90 mg/dL, and creatinine is 0.5 mg/dL. Upper gastrointestinal radiography series demonstrates a radiolucent filling defect in the pre-pyloric region. Of the following, the MOST likely diagnosis is: A. antral web B. chronic intestinal pseudo-obstruction C. duodenal stenosis D. Hirschsprung disease E. pyloric stenosis 2004/question 22
Board Review: Gastroenterology Antral webs are thin membranous diaphragms in the prepyloric region of the stomach. They are very rare causes of gastric outlet obstruction and present most commonly in infants younger than 6 months of age. As with pyloric stenosis, infants develop nonbilious vomiting and may be irritable because of their inability to retain gastric contents, as reported for the child in the vignette. Contrast radiography or ultrasonography demonstrates a linear density within a fluid-filled stomach. Like pyloric stenosis, the vomiting of gastric contents may be sufficiently severe to cause a hypochloremic alkalosis. However, the pyloric channel in a patient who has an antral web is normal (not thickened or elongated). Nonobstructing antral webs may be diagnosed in older children when they are being evaluated radiographically for abdominal pain, nausea, or weight loss. Treatment usually involves surgical lysis of the web, although endoscopic therapy theoretically is possible.Hypertrophic pyloric stenosis is a far more common cause of gastric outlet obstruction and hypochloremic alkalosis in a 2-month-old than antral web. The incidence may be as high as 1 in 500 live births. Infants typically present before the age of 3 months with progressive projectile nonbilious vomiting. If the lesion is not promptly diagnosed, infants may progress to dehydration, malnutrition, and hypochloremic alkalosis. Diagnosis is made either by an upper gastrointestinal radiographic series which identifies gastric outlet obstruction and a thickened pyloric channel or ultrasonography. Pyloric ultrasonography demonstrating a pyloric canal more than 18 mm in length or a pyloric muscle thickness of greater than 4 mm is diagnostic. Therapy consists of surgical pyloromyotomyDuodenal stenosis occurs when a membrane is present across the duodenal lumen in a manner similar to duodenal atresia. Patients who have Down syndrome are at increased risk for the development of both duodenal atresia and duodenal stenosis. Unlike pyloric stenosis or antral web, this condition presents with bilious vomiting, and abdominal imaging may demonstrate a dilated stomach and duodenum. Hirschsprung disease involves aganglionosis of a segment of colon (usually the rectosigmoid colon), leading to an inability to pass bowel contents. Affected neonates present with bowel obstruction and bilious vomiting; older children present with intractable chronic constipation. Intestinal pseudo-obstruction is a broad term referring to a group of myopathic and neuropathic conditions that impair bowel peristalsis.Patients present in infancy with abdominal distension, vomiting, and chronic constipation. Associated impairment of bladder function is seen in some patients. An abdominal plain film may identify air-fluid levels; an upper gastrointestinal with small bowel radiographic series fails to identify an anatomic explanation for the symptoms. This condition may persist into adulthood, and children may require parenteral nutrition.
Board Review: Gastroenterology 15 You are monitoring a 6-month-old male infant who has a history of direct hyperbilirubinemia, growth failure, and pruritus. A liver biopsy at 4 months of age demonstrated a paucity of intrahepatic bile ducts. On physical examination today, the child is alert and interactive but visibly jaundiced. His height is at the 5th percentile, and weight is below the 5th percentile. He appears mildly dysmorphic, having wide-spaced eyes and a small, pointed chin. Of the following, the additional physical finding that is MOST likely to be identified in this child is: A. Coloboma B. cutaneous hemangioma C. genu valgum D. perianal skin tags E. systolic heart murmur 2004/question 54
Board Review: Gastroenterology The paucity of intrahepatic bile ducts on liver biopsy reported for the infant in the vignette suggests the diagnosis of Alagille syndrome, which is associated with systolic heart murmurs.Alagille syndrome is an autosomal dominant genetic condition characterized by five principal features: paucity of the intrahepatic bile ducts, cardiac defects (especially peripheral pulmonic stenosis), posterior embryotoxon, vertebral anomalies (especially hemivertebrae), and peculiar facies (hypertelorism, pointed chin). Other conditions reported in Alagille syndrome include renal abnormalities (horseshoe kidney, tubular dysfunction) and ear abnormalities (otitis media, deafness). Infants usually are both short and underweight. Affected children are either cognitively normal or have mild developmental delay. Alagille syndrome typically presents with neonatal cholestasis (direct hyperbilirubinemia) in the first 3 months after birth. Physical examination demonstrates a thin, jaundiced infant. The systolic heart murmur of peripheral pulmonic stenosis typically is audible; echocardiography can identify other lesions. Laboratory studies demonstrate an increase in direct bilirubin, alkaline phosphatase, and gamma-glutamyl transpeptidase. Ophthalmologic examination is needed to demonstrate the posterior embryotoxon, which is a thickening of Schwalbe line (where the corneal endothelium and uveal trabecular meshwork meet). Chest radiography identifies hemivertebrae.Liver biopsy often is necessary to differentiate Alagille syndrome from other causes of neonatal cholestasis (eg, biliary atresia, alpha-1-antitrypsin deficiency).The prognosis of Alagille syndrome is highly variable and usually reflects the severity of the liver and cardiac disease. Approximately 20% to 25% of patients develop progressive severe liver disease that may require liver transplantation. Management is primarily supportive and involves aggressive nutritional supplementation in infants who are not growing; monitoring of fat-soluble vitamin levels; and supplementation with vitamins A, D, E, and K.Coloboma, cutaneous hemangioma, genu valgum, and perianal skin tags are not associated with Alagille syndrome.
Characteristic Alagille face of the patient (A, B) and his daughter (C, D). Note triangular shape, prominent forehead, deep-set eyes, broad nasal bridge, and pointed chin.
Board Review: Gastroenterology 16 • A 4-year-old boy has had abdominal cramps and diarrhea of 3 weeks' duration. Ten days prior to the onset of symptoms, he was treated with amoxicillin for streptococcal pharyngitis. The child's mother also has diarrhea and also was treated with amoxicillin. The boy's 2-month-old sibling, who is bottle-fed with cow milk formula, has had loose bowel movements. Stool cultures from all three family members are negative for Salmonella, Shigella, Yersinia, and Campylobacter sp as well as Escherichia coli 0157:H7. However, all samples are positive for Clostridium difficile toxin.Of the following, the MOST appropriate management of this mother and children is to: A. observe and follow all three patient B. treat all three patients with metronidazole C. treat the child only with metronidazole and observe the mother and infant D. treat the infant only with metronidazole and observe the mother and child E. treat the mother and child with metronidazole and observe the infant 2004/question 70
Board Review: Gastroenterology Both the mother and the 4-year-old child in the vignette have developed diarrhea associated with antibiotic therapy and show evidence of Clostridium difficile toxin in their stools. Because they are both symptomatic after the cessation of antibiotics, both should be treated with metronidazole to eradicate C difficile. The infant, however, probably is a carrier of C difficile, and therapy is not necessary. Colonization with C difficile occurs in 25% or more of infants younger than 6 months of age compared with 3% or fewer of children older than 18 months of age.C difficile is a gram-positive, spore-forming anaerobe that can cause colitis, particularly if the host's normal flora are eradicated with antibiotics. The clinical manifestations may range from asymptomatic carriage to mild diarrhea to severe bloody diarrhea. In more severe cases, sigmoidoscopy identifies white exudative plaques (pseudomembranes) overlying the colonic mucosa. C difficile is a nosocomial pathogen that is very difficult to remove from the hospital environment because the spores may be dormant on the floors, shelves, and windowsills of hospital rooms. Because culture of the organism is difficult, the diagnosis is established by identification of one of two toxins (toxin A or toxin B) in the stool. Currently, most laboratories use enzyme-linked immunosorbent assay to identify toxin.Asymptomatic carriage of C difficile is common in infants. Despite the presence of toxin in the stool, infants rarely become symptomatic or develop colitis from C difficile infection. For this reason, treatment of infants younger than 6 months of age is not warranted unless there is strong evidence that C difficile is causing the diarrhea.Treatment consists of oral metronidazole (5 to 10 mg/kg per dose tid for 10 days) or oral vancomycin (10 mg/kg per dose tid for 10 days). Because it is difficult to eradicate the spores of C difficile, recurrences are common. Recurrences may be treated either with longer antibiotic courses and a gradual tapering of therapy or with the addition of a probiotic such as Saccharomyces boulardii.
Board Review: Gastroenterology 17 • A 14-year-old boy presents with a history of growth failure, intermittent abdominal pain, and diarrhea. He was sent home from the emergency department last night after laboratory evaluation revealed a hematocrit of 32% (0.32), white blood cell count of 12 x 103/mcL (12 x 109/L), and erythrocyte sedimentation rate of 35 mm/h. You suspect inflammatory bowel disease.Of the following, the physical finding that is MOST likely to be associated with Crohn disease instead of ulcerative colitis is: A. arthritis of the left knee B. erythema nodosum C. perianal abscess D. short stature E. uveitis 2004/question 182
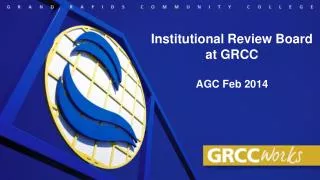
Board Review: Gastroenterology Inflammatory bowel disease of childhood typically is categorized into two conditions: ulcerative colitis (UC) and Crohn disease (CD). UC is characterized by inflammation limited to the mucosal layer of the colon. It may involve the rectum only, the left side of the colon, or the entire colon, but it does not involve the small intestine. In contrast, CD is characterized by transmural intestinal inflammation that may involve any portion of the intestinal tract from the mouth to the anus. The most common regions of involvement are the terminal ileum and the cecum. Perianal involvement, such as perianal fistula or abscess, is identified in up to 30% of patients who have CD, but it is not seen in patients who have UC.Arthritis, erythema nodosum, and uveitis are extraintestinal manifestations associated with both CD and UC.Growth failure and short stature occur in 50% of patients who have CD and 10% of patients who have UC.The diagnosis of inflammatory bowel disease most often is suspected when a patient either has bloody diarrhea with negative stool cultures or a constellation of other less specific findings (eg, abdominal pain, diarrhea, weight loss, anemia, fever, or arthralgias). Examination may identify short stature, oral ulcers, arthritis, skin lesions (eg, erythema nodosum), or perianal disease. Laboratory studies may demonstrate anemia, hypoalbuminemia, and an elevated erythrocyte sedimentation rate.Serologic testing for perinuclear antineutrophil cytoplasmic antibodies (pANCA) and anti-Saccharomyces cerevisiae antibodies (ASCA) also may suggest CD or UC, but the low sensitivity of this serologic testing limits its usefulness.The diagnosis is established by a combination of barium radiography, colonoscopy, and upper endoscopy. Ideally, the terminal ileum should be examined during the colonoscopy; patients who have ileal involvement exhibit deep fissuring ulcers, The identification of small bowel disease, perianal involvement, or granulomas on biopsy firmly establishes a diagnosis of CD instead of UC.
Erythema Nodosum: an acute, nodular, erythematous eruption that usually is limited to the extensor aspects of the lower legs. Chronic or recurrent EN is rare but may occur. EN is presumed to be a hypersensitivity reaction and may occur in association with several systemic diseases or drug therapies, or it may be idiopathic. The inflammatory reaction occurs in the panniculitis.
Crohn’s ileitis Normal Terminal Ileum Cobblestone appearance suggests transmural inflammation