Video Capsule Endoscopy
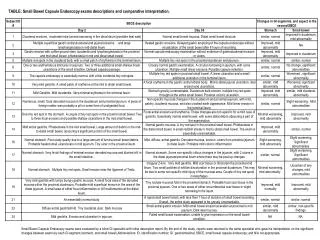
Video Capsule Endoscopy. Cem KALAYCI Marmara University Head, Dept. of Gastroenterology ESGAR, Istanbul 2008. Small Intestinal Capsule. Comparative Capsule Designs. VCE. PillCam (PillCam SB). (Given Imaging; Yoqneam, Israel): FDA Approval 2000. EndoCapsule (Olympus): FDA Approval 2007

Video Capsule Endoscopy
E N D
Presentation Transcript
Video Capsule Endoscopy Cem KALAYCI Marmara University Head, Dept. of Gastroenterology ESGAR, Istanbul 2008
VCE • PillCam (PillCam SB). (Given Imaging; Yoqneam, Israel): FDA Approval 2000. • EndoCapsule (Olympus): FDA Approval 2007 • Similar characteristics to the PillCam SB but has a CCD chip instead of a CMOS chip.
Given vs Olympus • 51 patients with obscure GI bleeding • PillCam SB and the EndoCapsule 40 minutes apart in randomized order • Similar results for normal and abnormal Gastrointest Endosc 2007; 65:AB125.
Technics • Two images per second • 55,000 images over eight hours. • Magnification 1:8 • Review of the video, generation of a report: 30 to 90 minutes. • Viewing: 1-25 frames per second (standard video speed).
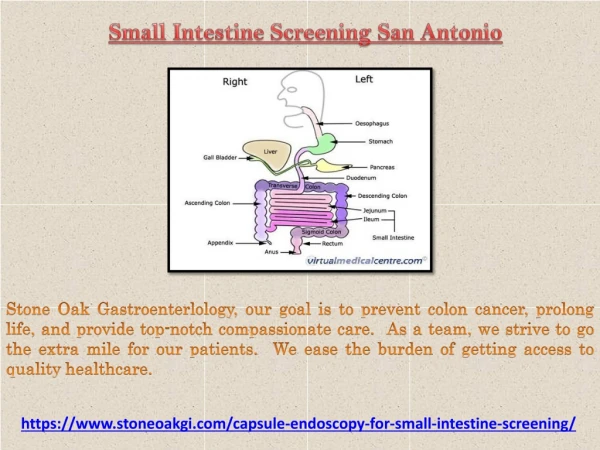
Primary Indications • Obscure gastrointestinal bleeding • Suspected Crohn's disease • Small bowel tumors
Other Indications • NSAID injury to the small bowel • Abdominal pain (functional vs organic) • Celiac disease
Additional Applications • Small bowel polyps • Rejection in small bowel transplantation • GVH diseaase after bone marrow transplantation • Surveillance of patients with hereditary polyposis syndromes.
Advantages • Noninvasive • Examination of the majority of the small bowel mucosa, which is not possible with push enteroscopy • Small bowel series, enteroclysis, and intra-operative enteroscopy are capable of examining the entire length of the small bowel, they are either quite insensitive or invasive.
Disadvantage • No tissue sampling or therapeutic intervention.
Obscure Bleeding(100 patients) n Pos.Study (%) • Ongoing overt bleeding 26 92 • Previous overt bleeding 31 13 • FOBT + and IDA 43 44 Pennazio et al, Gastroenterology 2004;126:643.
MOST COMMON FINDINGS • Angioectasia (29 percent) • Crohn's disease (6 percent). • Diagnostic yield is highest when performed as close as possible to the bleeding episode. Pennazio et al, Gastroenterology 2004;126:643.
Obscure Bleeding • Sixty-two patients underwent further examination that led to independent verification of the diagnosis in 56. • Sensitivity: 89 %, Specificity: 95 % • PPV: 97 % NPV: 83 % • Ongoing obscure bleeding (overt or occult) are the best candidates Pennazio et al, Gastroenterology 2004;126:643.
Video Capsule Endoscopy vs Push Enteroscopy in the Diagnosis of Obscure GI Bleeding
Yield in Obscure bleeding • A meta-analysis of 14 studies: • Capsule endoscopy: (63 percent) • Push enteroscopy (26 percent), • Barium studies (8 percent) Triester, SL et al. Am J Gastroenterol 2005; 100:2407.
VCE vs SBFT • 22 patients suspected of having small bowel pathology, underwent both VCE and SBFT. • Diagnostic study: VCE: 45 % SBFT: 20 % • Finding the cause of Obscure bleeding: VCE: 31% SBFT: 5 % Costamagna, G, et al. Gastroenterology 2002;123:999.
VCE vs DBE • Diagnosing the etiology: VCE: 80 % DBE: 60 % • A procedure/treatment was performed in 77 % of the patients with DBE • 74 % of the patients remained stable during 5 month follow up Hadithi M, et al. Am J Gastroenterol 2006:100 :1-6
Crohn’s Disease n VCE Push Entero Crohn’s 22 17 3 4 Suspected CD 21 4* 0 1 (false) *2 were false diagnosis Chong et al, Gastrointest Endosc 2005;61:255-61
Crohn’s Disease • VCE detected more erosions than push entero and enteroclysis (p<0.001) • There was no difference in patients with suspected Crohn’s disease. • Capsule endoscopy had a higher yield than push enteroscopy and enteroclysis in patients with known Crohn's disease Chong et al, Gatsrointest Endosc 2005;61:255-61 Marmo, R, et al. Clin Gastroenterol Hepatol 2005; 3:772.
Video Capsule Endoscopy and the Diagnosis of Suspected Crohn’s Disease
VCE vs Barium in suspected Crohn’s recurrence • Studies produced complementary results • VCE: Mucosal disease in six patients with a normal SBFT • SBFT: Grade 1 mucosal disease in five patients with a normal VCE study. Buchman, AL, et al. Am J Gastroenterol 2004; 99:2171.
Risk: Retention of the capsule • Clinically important retention < 1 %. • Patients with increased risk • known or suspected Crohn's disease • intermitent SB obstruction secondary to adhesions • radiation enteritis • severe motility disorders • Zenker's diverticulum. • A normal barium study or CT scan does not exclude the possibility of retention.
Capsule Retention • Palpation by the surgeon of the capsule retained above a stricture may be helpful in localizing the stricture, which may have no serosal signs, thus avoiding the need for intra-operative enteroscopy. • Removal of the retained capsule by double balloon enteroscopy has also been described
Patency capsule • Same size as the PillCam • Composed of lactose and barium • Contains a radiofrequency identification tag that allows it to be detected by a scanning device • Dissolves in 40 to 80 hours after ingestion.
Patency capsule • To assure small bowel patency before VCE • Diagnostic test for suspected small bowel strictures that cannot be identified by standard radiographic means. • 25 percent of patients with strictures developed abdominal pain, some severe, and two patients required emergency surgery Delvaux, M, V, et al. Endoscopy. 2005; 37:801.
Contraindications • Dementia • Gastroparesis (the capsule can be placed in the duodenum by endoscopy) • Esophageal stricture, swallowing disorders (eg, Zenker's diverticulum) (endoscopic placement)
Contraindications • Partial or intermittent small bowel obstruction • Those who are inoperable or refuse surgery • Patients who have defibrillators or pacemakers. This is a recommendation in the package insert, but does not appear to be a significant clinical problem.