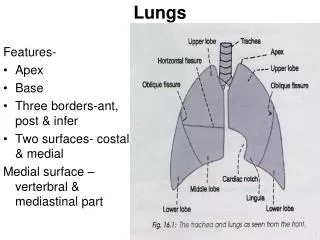
Chest and Lungs
670 likes | 952 Vues
Chest and Lungs. Adapted from Mosby’s Guide to Physical Examination, 6 th Ed. Ch. 13. Newborns. Obligate Nose Breathers Only open their mouth to breathe if in respiratory distress Rely primarily on the diaphragm for respiratory effort Commonly use abdominal muscles

Chest and Lungs
E N D
Presentation Transcript
Chest and Lungs Adapted from Mosby’s Guide to Physical Examination, 6th Ed. Ch. 13
Newborns • Obligate Nose Breathers • Only open their mouth to breathe if in respiratory distress • Rely primarily on the diaphragm for respiratory effort • Commonly use abdominal muscles • Gradually adding intercostal muscles
Newborns • Coughing • Rare • Should be considered a problem • Sneezing • Frequent and expected • Clears the nose
Newborn • Chest is generally round • A-P diameter approximately the same as the transverse • Chest circumference is approximately the same as the head circumference • Until ~2 years of age *With growth, the lateral diameter will eventually exceed the A-P diameter (adult)
Infant and Young Child • Bony structure is more prominent than the adult • Relatively thin chest wall • More cartilaginous and yielding • Xiphoid process is often more prominent and a bit more moveable
APGAR SCORE • Developed by Dr. Virginia Apgar (1953) • Subjective qualitative evaluation • done at 1 and 5 minutes • determine “survivability” of the newborn by observing the level of function of 5 components • Heart rate • Respiratory rate • Muscle tone • Reflex irritability • Color A ctivity P ulse G rimace A ppearance R espirations
A newborn whose respirations are inadequate but who is otherwise normal… • may initially score 1 (or even 0) on • heart rate • muscle tone • irritability • color
Depressed Respiration Origins: • Maternal environment during labor • Sedatives • Compromised blood supply to the child • Mechanical obstruction by mucus What about… Neurological damage (birth trauma)?
Infant Chest & Lung Exam • Similar to the adult exam • Inspecting without disturbing the baby is key • Percussion is usually unreliable • Examiner’s fingers may be too large
Inspect thoracic cage • Size • Shape • Measure chest circumference • Full-term infant: 30-36 cm • Sometimes 2-3 cm smaller than head circumference • Increases with prematurity
Intrauterine growth retardation • Smaller chest circumference compared to the head Poorly controlled diabetes • Relatively larger chest circumference
Measure distance between the nipples • ¼ chest circumference • Note: • Symmetry in size • Supernumerary • Swelling • Discharge Breast development in a newborn -d/t hormonal influences
Respiratory Rate • Count for 1 minute • Average: 40-60 rpm • though 80 rpm is not uncommon • If room temp is very warm or cool, variation in the rate occurs • Most often tachypnea • Sometimes bradypnea
Rhythm • Note regularity of respiration • Premature infants are more likely to have irregular respiratory patterns • Periodic breathing • sequence of relatively vigorous respiratory efforts followed by apnea of as long as 10-15 seconds
Periodic Breathing Cause for concern if … • Apneic episodes tend to be prolonged • Baby becomes centrally cyanotic • In the term infant periodic breathing should wane a few hours after birth • Persistence in preterm infants is relative to gestational age • Apneic periods should diminish in frequency as they approach term status
CLINICAL NOTE Newborn • Pattern of respirations will vary with room temperature, feeding and sleep • During the first few hours… respiratory effort may be depressed by passive transfer of drugs given to the mother before delivery
If chest expansion is asymmetric suspect inability to fill one of the lungs • Pneumothorax • Presence of air/gas in the pleural cavity • Diaphragmatic hernia
Palpate • Rib cage and sternum • Loss of symmetry • Unusual masses • Crepitus • Fractured clavicle (birth trauma) • May show no evidence of pain • Xiphoid • Mobile and prominent • Sharp inferior tip; move back and forth under your finger
Auscultation Wait for quiet!
Auscultation • Localization of breath sounds is difficult • Difficult to detect absence of breath sounds in any given area • Breath sounds are easily transmitted from one segment to another
Movement • Mucus in the upper airway • Gurgling (intestinal tract) …may contribute to adventitious sounds making evaluation difficult • If GI gurgling sounds are persistently hears in the chest • Suspect diaphragmatic hernia
Crackles and Ronchi • Not uncommon immediately after birth • Fluid has not completely cleared • If asymmetric… • a problem should be suspected • aspiration of meconium
Stridor • High pitched, piercing sound • Most often heard during inspiration • Obstruction high in the respiratory tree *Cannot be dismissed as inconsequential • Especially when inspiration is longer than expiration
If accompanied by cough, hoarseness or retraction you must consider a serious problem in trachea or larynx… Differentials include: • Floppy epiglottis • Congenital defects • Croup • Edematous response • Infection • Allergen • Smoke • Chemicals • Aspirated foreign body
Respiratory Grunting • Infant tries to expel trapped air or fetal lung fluid while trying to retain air and increase oxygen levels If persistent, cause for concern.
Increased Respiratory Effort • Retraction at the supraclavicular notch • Contraction of the SCM’s • Flaring of the nostrils (alae nasi) *Should be considered significant. See-saw respirations
Use thoracic (intercostal) musculature for respiration by age 6 or 7 • Obvious intercostal exertion (retractions) suggests a problem • Respiratory rates that exceed the indicated limits also suggest difficulty
Assessing Respiratory Distress • Does a loss of synchrony between L and R occur during the respiratory effort? Is there a lag in movement of the chest on one side? Atelectasis? Diaphragmatic hernia? • Is there stridor? Croup? Epiglottitis? • Is there retraction at the suprasternal notch, intercostally, or at the xiphoid process? • Do the nares dilate and flare with respiratory effort? Is pneumonia present? • Is there an audible expiratory grunt? Is it audible with the stethoscope only or without? Is there lower airway obstruction? Focal atelectasis? • Is there paradoxic breathing?
Crying Child… Seize the opportunity! • A sob is frequently followed by a deep breath • Allows the evaluation of vocal resonance • Feel for tactile fremitus • Whole hand, palm and fingers
<5 years old • May not be able to give enough of an expiration to satisfy you • Especially with subtle wheezing • Ask them to “blow out” your penlight or to blow away a bit of tissue in your hand • Listen after they run up and down the hallway
Chest wall is thinner and more resonant than adult’s • Intrathoracic sounds are easier to hear • Hyperresonance is common • Easy to miss the dullness of underlying consolidation (percussion) If you sense some loss of resonance, give it as much importance as you would give frank dullness in the adult.
Child Because the chest wall is thinner… • Breath sounds may sound louder, harsher, and more bronchial Bronchovesicular sounds may be heard throughout the chest.
Persistence of “Barrel Chest” • If the “roundness” of a child’s chest persists past the 2nd year • Possible chronic obstructive pulmonary problem • Cystic fibrosis
Asthma • Chronic obstructive pulmonary disease (COPD) characterized by airway inflammation • Hyperreactivity to: • Allergens • Anxiety • URTI • Smoke • Exercise • Cold air
Results in: • mucosal edema • increased secretions • bronchoconstriction Airway resistance increases and respiratory flow is impeded.
Episodes are characterized by: • Paroxysmal dyspnea • Tachypnea • Cough • Wheezing (expiration & inspiration) • Prolonged expiration • Chest pain/tightness
Episodes may last for just minutes or hours, or they may be prolonged over days • ANXIETY • Can be life threatening though usually reversible • spontaneously or in response to therapy • Between episodes, the patient my be completely asymptomatic
Note… A wheezing patient withgeneralized pulmonary findingsmay haveasthma or a viral infection, but rarely, if ever, a bacterial infection.
Atelectasis Lung is airless… • Incomplete expansion of the lung at birth OR • Collapse of the lung at any age • Compression from outside • Exudates, tumors • Resorption of gas from the alveoli with complete internal obstruction
Bronchiolitis Viral; respiratory syncytial virus (RSV) Most common: <6 months • Expiration becomes difficult • Hyperinflation of lungs • Increased A-P diameter of thoracic cage • Hyperresonant percussion
Infant appears anxious • Tachypnea • Rapid and short breaths; expiratory phase prolonged • Generalized retraction • Perioral cyanosis • Abdomen appears distended (swallowed air) • Possible wheezing and crackles
Bronchitis Initial stimulus = irritation (Internal or external) • Inflammation of the mucus membranes of the bronchial tubes
Acute bronchitis • Fever and chest pain • May be more or less severe than chronic • Chronic bronchitis • Variety of causes and physical manifestations • Excessive secretion of mucus in the bronchial tree • Both can show varying degrees of involvement • Possible obstruction and even atelectasis • Most often quite mild