MERS- CoV
MERS- CoV. Presentor : Norlida Binti Suhaimi Moderator : Dr Khairuddin Bin Ismail Dr Nik Azman Bin Nik Adib. MERS-COV. Dr Benedict Sim Infectious disease physician Hosp Sg Buloh. Dr. Wan Noraini ; Surveillance Section, Disease Control Divisio n


MERS- CoV
E N D
Presentation Transcript
MERS-CoV Presentor : Norlida Binti Suhaimi Moderator : Dr Khairuddin Bin Ismail Dr Nik Azman Bin Nik Adib
MERS-COV Dr Benedict Sim Infectious disease physician Hosp Sg Buloh Dr. Wan Noraini ; Surveillance Section, Disease Control Division Dr. Shahanizan bt Mohd Zin; Medical Development Division Dr Anilawati ; ID Physician, Kota Bahru
Outline • What will MERS-CoV look like? • Who has MERS-CoV? • Who do test? • How do test? • When to admit? • Where to admit? • What infection control needed? • How to treat ?
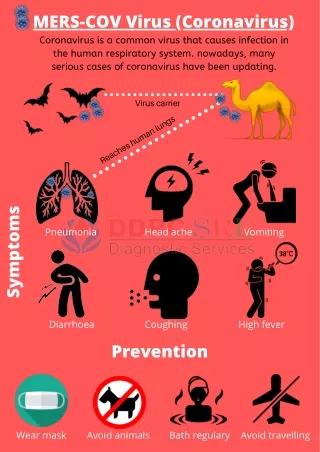
Introduction… • Coronaviruses : - large family of viruses that can cause a range of illnesses in humans - from the common cold to severe acute respiratory syndrome (SARS). - cause disease in a wide variety of animal species.
In late 2012, a novel coronavirus that had not previously been seen in humans was identified for the first time in a resident of the Middle East - known as the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) • Thus far, all patients infected with MERS-CoV have had a direct or indirect link to the Middle East
however, local non-sustained human-to-human transmission has occurred in other countries, in people who had recently travelled to the Middle East. • The MERS-CoV virus is thought to be an animal virus that has sporadically resulted in human infections, with subsequent limited transmission between humans.
MERS – CoV : genetic similarity to viruses previously described in bats. • However, even if an animal reservoir is identified, it is critical to identify the types of exposures that result in infection and the mode of transmission. • It is unlikely that transmission occurs directly from animals to humans • route of transmission may be complex requiring intermediary hosts, or through contaminated food or drink.
Human-to-human transmission has occurred in health care settings, among close family contacts, and in the work place. • Sustained transmission in the community beyond these clusters has not been observed and would represent a major change in the epidemiology of MERS-CoV.
Pt characteristics (as of 7.6.13) Male to female ratio 2.6 : 1.0 Median age 56 years (range: 2–94 years) All aged >24 years, except 2 children(2 & 14 yrs) Deaths: Case fatality rate = 31/55 = 56% 4~14d after onset, 2~10d after hospitalization
23 confirmed cases in Eastern Saudi Arabia 20/23 (87%) 20/23 (87%) 11/23 (48%) 8/23 (35%) 5/23 (22%) 4/23 (17%) 20/23 • fever • cough • shortness of breath • gastrointestinal symptoms • diarrhoea • vomiting • abnormal CXR
Clinical symptoms • Most - pneumonia. Some - GI symptoms, diarrhoea • 1 immuno-compromised patient - fever and diarrhoea; pneumonia only on CXR. • Half have died. • Complications • respiratory failure • ARDS with multi-organ failure • renal failure requiring dialysis • consumptive coagulopathy • pericarditis. • Co-infections - influenza, herpes simplex, and pneumococcus
The date of onset was defined: • among febrile patients as the first day of fever that persisted for more than 48 hours • afebrile patients as the first day of new cough or shortness of breath.
As of June 12… - 15 patients (65%) died - 6 patients (26%) had recovered - 2 patients (9%) remained hospitalized. • A total of 21 of the 23 cases were acquired by person-to-person transmission in hemodialysis units, intensive care units, or in-patient units in three different health care facilities.
Among 217 household contacts and more than 200 health care worker contacts whom identified - MERS-CoV infection developed in 5 family members (3 with laboratory- confirmed cases) - and in 2 health care workers (both with laboratory-confirmed cases).
Incubation period • Where exposure is known or strongly suspected - generally < 1/52 • In at least one case, 9 to 12 days. • In a minority of cases, may exceed one week but is less than 2 weeks
Important findings Coinfection with influenza & parainfluenza - ? Roles in transmissibility and/or the severity of the illness. Transmissibility pattern ? SARS Reported case of milder nCoV illness – spectrum of clinical disease maybe wider Limited person-to-person transmission Settings: Hospital, Household Most family members and HCWs closely exposed did not develop disease No evidence at present of sustained person-to-person transmission
Susceptibility Undetermined Presumably universal Presumable vulnerability in elder people with pre-existing medical condition Lower risk for children and women?
Route of transmission Undetermined Droplet and direct contact probably Large droplet transmission is suspected as the most likely route. B Guery et al. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: a report of nosocomial transmission. Lancet (2013).
MOH/WHO Case definition… Confirmed Case: lab confirm Probable Case: • SARI* with clinical, radiological, or HPE evidence of pulmparenchymal ds [e.g. pneumonia or ARDS]; AND • no possibility of lab confirmation AND • close contact** with lab-confirmed case. *Include hxof fever or measured fever **Close contact – anyone who - Provided care for the pt, including HCW or family member; - Stayed at the same place (e.g., lived with, visited) while pt ill
WHO Interim case definition 1) Confirmed case • A person with laboratory confirmation of MERS-CoV infection. • molecular diagnostics including either +ve PCR on at least two specific genomic targets or a single +ve target with sequencing on a second. 2) Probable case
Probable case… • Febrile ARI with clinical, radiological, or HPE evidence (C/R/HPE) of pulm parenchymal ds (PPD) e.g. pneumonia or ARDSAND Testing for MERS-CoV - unavailable / negative on a single inadequate specimen AND Direct epid-link with a confirmed MERS-CoV case • Febrile ARI with C/R/HPE of PPD ANDInconclusive MERS-CoV(+ve screening test w/out confirmation)AND A resident of or traveler to Middle East 14/7 before onset of illness.
Febrile ARI of any severity ANDInconclusive MERS-CoV(+ve screening test w/out confirmation) ANDDirect epid-link with a confirmed MERS-CoV case.
Inadequate sp • NP swab without lower respsp, • sp with improper handling, • judged to be poor quality by lab, • taken too late. • A direct epid link may include: • Close physical contact • Working together in close proximity or sharing the same classroom environment • Traveling together in any kind of conveyance • Living in the same household • 14/7 period before or after the onset of illness in the case under consideration.
Inconclusive tests : • A positive screening test without further confirmation eg positive on a single PCR target • A serological assay positive.
Inconclusive testing: • Should undergo additional virologic and serologic testing. • Strongly advised that lower resp sp such as sputum, ET aspirate, or BAL be used. • If no S&S of LRTI and lower track sp not available or clinically indicated, bothNP and OP swab sp should be collected. • If NP swab is negative in a pt strongly suspected to have MERS-CoV infection, retest using a lower resp sp or a repeat NP sp with additional OP sp and paired acute and convalescent sera.
Pt Under Ix • SARI, (include history of fever and cough) and indications ofPPD (e.g., pneumonia or ARDS), based on clinical or radiological evidence of consolidation, (possibility of atypical presentations in immunocompromised) AND • Travel to the Middle East 10/7 before AND • Not explained by other aetiology
Contacts • ARI of any severity, • 10 days before onset of illness, • close physical contact* with a confirmed or probable case of MERS-CoV infection • HCW • working where pt with SARI cared for, (esp ICU) • without regard to history of travel (WRTHOT) • Not explained by other aetiology
Objectives of screening 1. Detect early, sustained human-to-human transmission.2. Determine the geographic risk area for infection with the virus.Clinical and epidemiological Ix to:1. Determine clinical characteristics - incubation period, spectrum of disease, and natural history. 2. Determine epidemiological characteristics - exposures that result in infection, risk factors, secondary attack rates, and MOT
Who should be investigated?- summarized • SARI + PPD + either • In a cluster (within 14/7) • HCW exposed to pt with severe LRTI • Traveled to middle east - 14/7 • unexpected clinical course unexplained by current aetiology • ARI of any severity • close contact with confirmed/probable MERS-CoV within 14/7 • Middle East, any ventilated pt
SARI + PPD +either • cluster(>1 persons in a specific setting -classroom, workplace, household, extended family, hospital, other residential institution, military barracks or recreational camp) that occurs within 14-days, WRTHOT unless another aetiology identified (UAAI). • HCW working with severe ARI patients (particularly ICU) WRTHOT UAAI
travel to the Middle East within 14 days before onset of illness, UAAI. • unusual or unexpected clinical course, especially sudden deterioration despite appropriate treatment, WRTHOT , even if another aetiology has been identified, if it does not fully explain the presentation or clinical course of the patient.
WHO update… • Stronger recommendations for lower respiratory specimens, rather than NP swabs, to be used to diagnose MERS-CoV infection. • A longer period of observation for contacts of cases.
NP swabs are not as sensitive as lower respiratory specimens – BAL, tracheal aspirate, sputum • If patients do not have LRTI or specimens not possible, both NP and OP should be collected