MALIGNANT DIABETES AND ASSOCIATED MORTALITY
630 likes | 794 Vues
Learn about the factors contributing to diabetic foot ulcers and amputations, and how multidisciplinary teams can improve outcomes.

MALIGNANT DIABETES AND ASSOCIATED MORTALITY
E N D
Presentation Transcript
MALIGNANT DIABETES AND ASSOCIATED MORTALITY CAN WE DO ANYTHING ABOUT IT? Terri DeJohn, M.D. Medical Director Hyperbaric Medicine and Wound Treatment Center
OBJECTIVES Identify factors which contribute to increased mortality in the DFU patient. Learn who to call for help and when to make that call.
DIABETES IS INCREASING 26 million people in the U.S. have diabetes 1.9 million diagnosed in 2010 15% will develop Diabetic Foot Ulcers (DFU)
AMPUTATIONS 71% are toe, TMA and Symes amputations 82% decrease in BKA or AKA • 15% of DFU’s End in Amputation
AMPUTATION INCIDENCE IN MINORITIES per 10,000 Diabetics MEN have twice the incidence of amputation as women in all races
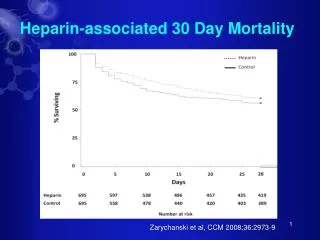
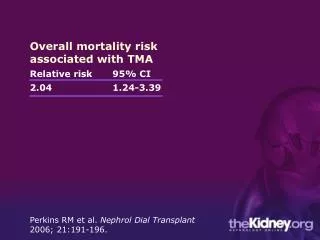
MALIGNANT DIABETES Armstrong DG. Int Wound J. 2007;Dec;4(4):286-7.
MORTALITY RISK IMPROVES WITH TREATMENT BY A MULTI-DISCIPLINARY TEAM In 5 Years Living Dead
MULTIFACTORIAL ETIOLOGY Diabetes Amputation
MULTIFACTORIAL ETIOLOGY Diabetes Amputation
MULTIFACTORIAL ETIOLOGY Amputation Vascular Disease Infection Ulceration Deformity • Neuropathy Diabetes
LIMB SALVAGE TEAM • Multiple problems contribute to critical wounds and potential amputation. • Multiple doctors with expertise in their area working together to save a leg.
MULTIFACTORIAL ETIOLOGY Amputation Vascular Disease - CV Infection - IMMUNE Ulceration - DERMATALOGIC Deformity- ORTHOPEDIC • Neuropathy - NEUROLOGIC Diabetes - ENDOCRINE
OUTCOMES OF MULTIDISCIPLINARY TEAMS
Moving from aWound Clinicor Lone Practitioner to a Limb Salvage Team
Rapid Referral to Multi-disciplinary Team Referral before 25 days resulted in a 79% reduction in amputations. • vanAcker, et al, DFCon2011 Establishing a National Diabetic Foot Model
RECOMMENDATIONS FROM EVIDENCE CONSENSUS RECOMMENDATIONS ON ADVANCING THE STANDARD OF CARE FOR TREATING NEUROPATHIC FOOT ULCERS IN PATIENTS WITH DIABETES APRIL 2010 OSTOMY AND WOUND MANAGEMENT
TREATMENT OF DFU’s DEFINE DISCUSS DEBRIDE (VESSELS AND BED) DEBUG DECIDE DE-LOAD
DEFINE SKIN AND ULCER EXAM • Skin • Sensation • Deformity • Ulcer: Size, Location, Base, Wound edge, Tunnel, Necrosis
DEFINE INFECTION • Drainage • Odor • Redness • Swelling • Probe Bone • If suspicious: ESR, CRP (If both are normal, Osteomyelitis is unlikely), Culture
IMAGING Plain films MRI or CT
VASCULAR EVALUATION A tiered approach is recommended : 1. Pulses, ABI, and/or TBI 2. Segmental pressure volume, SPP and TcPO2 3. Vascular consultation
TISSUE HYPOXIA TcPO2 < 40mmHg suggests impaired healing Risk of amputation is 161 times greater if TcPO2 <20 rather than TcPO2 >40 Risk amputation is 55 time greater if ABI is <0.45 rather than >0.7
DEFINE LABS CBC HgA1c Cholesterol, HDL, LDL Homocysteine (Hcy)
Effects of Hyperglycemia on Cells 1. Decreased proliferation and differentiation of keratinocytes (1) 2. Inhibition of fibroblast proliferation (2) 3. Decreased response of cells to growth factors (2,3) 4. Decreased migration of keratinocytes and fibroblasts (4) (1) Sparvchikov N, ed al. Diabetes 2001; 50: 1627-635 (2)Hehenberger K, et al. Cell BiochemFunct 1997; 15: 197-201 (3)Fard A, et al. ArteriosclerThromVascBiol 2000; 20: 2039-2044 (4)Lerman OZ, et al. Am J Pathol 2003; 162:303-312
HEMOGLOBIN A1C & WOUND HEALING Methods: A retrospective analysis of data gathered from multi-center, controlled, prospective, randomized FDA approved clinical trials is being conducted. Results: The final linear regression model (P<0.0001) found that higher HgbA1C levels were associated with lower percentages of wound healing (P=0.05). For every 1% increase in HgbA1c there is a decrease of 3% in expected healing area Hanft J, et al, South Miami Hospital & Harvard Medical School, APMA Scientific Meeting Abstract, 2009
DEFINE LABS CBC HgA1c Cholesterol, HDL, LDL Homocysteine (Hcy)
Homocysteine (Hcy) Known risk factor for atherosclerotic vascular disease and is an inhibitor of nitric oxide (NO) bioactivity ↑ Hcy was observed in 50% of patients with chronic wounds 63% of patients with diabetic, neuropathic ulcers
TREATMENT OF HYPER- Hcy METANX L-methylfolate Pyridoxal 5'-phosphate Methylcobalamin Results in 3X’s lower serum Hcy
DEFINE NUTRITION • Nutrition Screen • Albumin, Pre-Albumin, Transferrin CONSIDER PROTEIN SUPPLEMENTS .5 - .75 gm / kg of body weight
DEFINE SMOKING • Nicotine • Cyanide • Carbon Monoxide CONSIDER E-CIGARETTE
DEFINED DISEASE PROCESSES ULCER DEFORMITY INFECTION VASCULAR STATUS DIABETIC CONTROL NUTRITIONAL STATE
DEFINE & DISCUSS Initial definition to determine what issues contribute to the problem Discuss with appropriate specialists
DEFINE AND DISCUSS Tissue Hypoxia Deformity Infection Diabetic Control Nutrition Vascular surgeon Ortho/ Podiatry/ Pedorthotist Infectious Disease Endocrinologist/ Diabetic Ed Dietician
DEBRIDE • Debridement • Sharp • Mechanical • Chemical • Autolytic
BIOFILMS Biofilms are present in 60% of chronic wound biopsies Only 6% of Acute Wound Biopsies Biofilms retard wound healing Schierle WWR 17:2009
BIOFILMS Biofilms induce a chronic inflammatory response • Reactive Oxygen Species (ROS) • Proteases ( MMP, neutrophil elastase) Chronic inflammation leads to damage of proteins that are essential for healing. • Extracellular Matrix Proteins • Growth factors and receptors
DECIDE: WHAT DRESSING Wound care dressing orders for 202 patients receiving home health or HMO care 42% Wet-to-Dry 7.5% Enzymatic 7% Dry Gauze Cowan L, Stechmiller J. Advances in Skin and Wound Care Dec, 2009
DECIDE: WHAT DRESSING • TO DRY: • Alginates • Foams • ABD’s • Polymers • NPWT • TO MOISTEN: • Hydrogel • Medihoney • Ointments
DECIDE: WHAT DRESSING ANTIMICROBIAL Silver Iodosorb Medihoney ACTIVE DRESSING Collagens Regranex Skin Substitutes
DE-LOAD (Off- Load) OFF LOADING DEVICES
OFF LOADING TOTAL CONTACT CASTING Only device proven to effectively off load REMOVABLE DEVICES ARE REMOVED Only 28% of daily activity done with device Armstrong, Diabetes Care 2003
QUALITYCARE BENCHMARKING Off Loading is the #1 Benchmark Diabetic Control Vascular Exam
DECIDE @ 4 WEEKS A 50% reduction in wound area at 4 weeks is a surrogate marker predictive of wound healing. % Area Reduction at 4 weeks
Percentage of Area Reduction = (A1 - A2) ÷ A1 x 100 A = Length x Width
FAILURE TO ACHIEVE 50% CLOSURE @ 4 WEEKS REQUIRES ADVANCED THERAPIES