HORIZONS AMI Trial
HORIZONS AMI Trial. H armonizing O utcomes with R evascular IZ ati ON and S tents In A cute M ycoardial I nfarction. www.clinicaltrialresults.org. HORIZONS AMI H armonizing O utcomes with R evascular IZ ati ON and S tents in A cute M yocardial I nfarction.

HORIZONS AMI Trial
E N D
Presentation Transcript
HORIZONS AMI Trial HarmonizingOutcomes with RevascularIZatiONandStentsIn AcuteMycoardialInfarction www.clinicaltrialresults.org
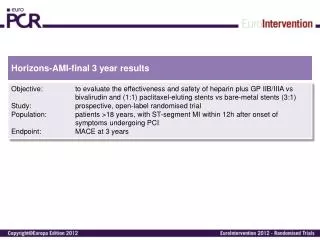
HORIZONS AMIHarmonizing Outcomes with RevascularIZatiON and Stents in Acute Myocardial Infarction • The Cardiovascular Research Foundation • PI: Gregg Stone, MD • Research Grants from Boston Scientific & The Medicines Company • A dual arm randomization trial in patients with ST segment elevation AMI (STEMI) to compare the results of using anticoagulation with either UFH plus routine GP IIb/IIIA inhibition with bivalirudin and bail-out GP IIb/IIIa inhibition, and primary angioplasty with stent implantation with either a slow rate-release paclitaxel stent (TAXUS) or an otherwise identical uncoated bare metal stent (Express) • Approx. 3600 patients in 200 global sites • Results on target to present at TCT 2007 www.clinicaltrialresults.org
HORIZONS AMI Trial 3400 randomized pts undergoing primary PCI Hypothesis:Bivalirudin compared to UFH + routine IIb/IIIa will reduce the composite rate of death, reinfarction, TVR, stroke and major bleeding at 30-days Anti-thrombotic therapy Randomize 1:1 Bivalirudin + bail-out IIb/IIIa UFH + IIb/IIIa inhibitor Hypothesis:Use of the polymer-based slow-release paclitaxel-eluting TAXUS stent will safely reduce the 1-year rate of ischemia-driven TLR Target vessel stentingRandomize 3:1 Bare metal Express stent TAXUS stent Sponsor: The Cardiovascular Research Foundation (PI: Gregg W. Stone), with unrestricted grant support from: Boston Scientific & The Medicine’s Co. www.clinicaltrialresults.org
Protocol Overview 3400 Patients with ST segment elevation AMI within 12 hours of symptom onset undergoing primary angioplasty Consent Aspirin 325 mg p.o. – Clopidogrel 300-600 mg p.o. – Ticlopidine 500 mg p.o. Drug Randomization rate 1:1 Unfractionated heparin + IIb/IIIa n=1700 Bivalirudin + bail-out IIb/IIIa n=1700 Stratification: • Non protocol pre-procedure heparin • 300mg clopidogrel load vs. 600mg clopidogrel load vs. 500mg ticlopidine load • IIb/IIIA: abciximab vs. eptifibatide • U.S. vs. non-U.S. site Cath lab – left ventriculography / coronary arteriography No FDA Approved PCI/CABG/Med Rx. TAXUS™ / Express™ stent eligible infarct lesion(s) (est ~ 88% = 3000)
Protocol Overview Stratification: • Result from first randomization • Medically treated diabetes • Intention to use overlapping stents • U.S. vs. non-U.S. sites Yes Infarcted vessel Randomization Rate 1:3 TAXUS™ Stent (n=2250) Bare metal control stent: Express™ (n=750) 1, 6, and 12 month follow-up for all patients undergoing primary randomization and then yearly for 5 years total for patients undergoing second randomization 1500 patients angiographic subset at 13 months (stent randomized patients only with successful procedure and no stent thrombosis or CABG up to 30 days) www.clinicaltrialresults.org
Protocol Procedures First Randomization Clinical Inclusion Criteria • At least 18 years of age (no upper age limit) • Clinical symptoms of AMI lasting >20 minutes and <12 hours (if <1 hour unresponsive to nitroglycerin) • ECG criteria: ST-segment elevation of ≥1mm in ≥2 contiguous leads, or (presumably new) left bundle branch block, or true posterior MI with ST depression of ≥1mm in ≥2 contiguous anterior leads • Patient or guardian agrees to study protocol and follow-up and provides IRB/EC approved written informed consent www.clinicaltrialresults.org
Protocol Overview Study Design (cont.) • First Randomization 1:1 n = 3,400 • UFH + IIb/IIIa inhibitor n = 1,700 • Bivalirudin + bail out IIb/IIIa n = 1,700 • Second Randomization 1:3 ~88% = 3,000 • Express™ stent n = 750 • TAXUS™ stent n = 2,250 • Follow-Up Visits Required: • 1, 6, and 12 months for all patients undergoing primary randomization • Angiography at 13 months for 1,500 stent randomized patients only • Yearly for 5 years for patients undergoing second randomization www.clinicaltrialresults.org
Protocol Overview • Pharmacology Arm Objectives • Establish safety and efficacy of bivalirudin in patients with AMI undergoing primary PCI by comparing to UFH plus routine use of IIb/IIIa inhibitors, bivalirudin result in: • Reduced rates of major bleeding events at 30 days • Similar rates or major adverse ischemic cardiac events at 30 days • Reduced rates of the composite of major adverse ischemic cardiac events + major bleeding at 30 days www.clinicaltrialresults.org
Protocol Overview • Stent Arm Objectives • Establish safety and efficacy of paclitaxel-eluting TAXUS™ stent by comparing to an otherwise identical bare metal Express™ stent will result in: • Reduced rates of target lesion revascularization for ischemia at 1-year • Similar rates of death, reinfarction, disabling stroke or subacute stent thrombosis at 1-year • Lower rates of in-stent and analysis segment binary angiographic restenosis at 13-months www.clinicaltrialresults.org