Download
1 / 55
550 likes | 733 Vues
Scientific Update of ADHD. Russell Schachar The Hospital for Sick Children Department of Psychiatry Brain and Behaviour Programme University of Toronto. Affiliations. CIHR Barr, Kennedy, Ickowicz, Crosbie, Pakulak, Ornstein Noseworthy, Chevrier Robaey, Perusse NINDS

E N D
Scientific Updateof ADHD Russell Schachar The Hospital for Sick Children Department of Psychiatry Brain and Behaviour Programme University of Toronto
Affiliations • CIHR • Barr, Kennedy, Ickowicz, Crosbie, Pakulak, Ornstein • Noseworthy, Chevrier • Robaey, Perusse • NINDS • Levin, Dennis, Barnes • Lilly • Purdue Frederick • Shire
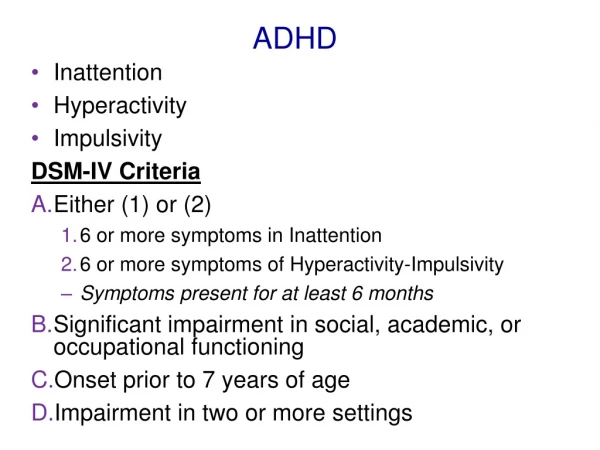
Outline • Summary and overview current understanding • Neuroscience 101 Genes Proteins Brain structure Cognitive function Behavior • Caveats
ADHD hyp-imp inattention function environment Cell membranes, transmitters, assemblies… Proteins g 1 g 2 g 3
What are genes? • DNA is specific sequence of nucleotide bases that encode instructions for proteins • Genome is complete set of DNA
How do genes function? • Many changes evident and passed on • Most changes cannot be seen by microscope • Most base pairs are not involved in genes and are not functional • Can be used to track functional changes • May regulate gene expression or function • Epigenetic factors affect gene function • Many hereditary effects may be outside of genes
Neurotransmitter systems • Serotonin • Noradrenalin • Glutamate • GABA • Transporters and receptors variably distributed Dopamine transporter
Dopamine D4 48bp Repeat Variants: Pharmacologic differences not linearly correlated with number of repeats EC50 Asghari et al, 1995 Jovanovic et al, 1999 2R 4R 7R 10R Implication: the 7R allele has a blunted response to dopamine
SNAP-25 • Critical for controlled release of neurotransmitters into the synaptic cleft • Loss of expression of a single copy of the gene results in dysregulation in the controlled release of glutamate, dopamine, and serotonin in select brain regions SNAP-25
Neural development • Stem cells differentiate • Growth factors (sonic hedgehog, notch, BDNF) • Half survive • Development depends of where they end up, activity there (use it or lose it!) • Rate of division/survival depends on experience, formation of synapses, integration into networks • Loss of neurons normal (exaggerated in some diseases) • Neurons likely regenerate and affected by experience (can teach old dog new tricks) • Environment can affect gene expression
Prefrontal cortex • Not involved in specific tasks • Executive control of behaviour, thought and affect • Organization and planning for future action and social goals • Balances perceptual, instinctual and motivational input • Reflective: guided by internal states and intentions • Control subordinate attention and motor processes
Prefrontal subcortical circuits • Begin and end in frontal cortex • Pass through subcortical structures • Reciprocal and interacting connections • Excitatory and inhibitory neurotransmitters • Separate yet overlapping and interacting • Specific and intermingled mixture of deficits • Evident in individuals with massive lesions
Dorsolateral circuit • Organization, planning, attention • Lesions generate concrete thinking, inability to stop, shift set, filter and ignore distractions, plan and organize
Orbitofrontal circuit • Mediates socially appropriate behaviour • Lesions lead to marked personality change, social disinhibition, explosiveness, tactlessness, lability, lack of interpersonal sensitivity
Anterior cingulate circuit • Motivation, balancing competing demands, performance monitoring • Lesions result in akinetic mutism, apathy, lack of motivation, insensitive to errors
Frontal/ executive processes“wave of attention” • Encoding, maintaining, retrieving in working memory • Preparing and anticipating • Interference management • Withholding of response tendency • Maintain set • Retract or inhibition • Error detection • Error correction
Summary • Considerable understanding of brain development and function • Differentiation in structure and function • Cognitive deficits • Genetic risks • Structural and functional anomalies
ADHD genetics • Highly genetic • Not simple Mendelian inheritance • Multigenic • Non-genetic factors contribute separately and through various combinations • Disorder occurs when combination of genetic and non-genetic factors exceeds some threshold • Nature of risk and mode of inheritance unknown
Genetics of ADHD % risk to family % concordance
Genome Scan Systematically screen all of the chromosomes for linkage using DNA markers spaced at regular intervals D19S229 D19S247 D19S204 D19S221 D19S179 D19S248 D19S178 D19S246 D19S180 D19S254
Genome scans for ADHD • Fisher et al., 2002 • UCLA 126 affected sib pairs • no regions met genome-wide significance levels • suggestive 5p12, 10q26, 12q23, 16p13 (Smalley, 2002) • Ogdie et al., 2003 • expansion of Fisher et al., sample + 144 sib pairs • 17p11 (LOD 2.98), 16p13 • Bakker et al., 2003 • 164 Dutch affected sib pairs • regions with LOD scores > 3, 15q15.1, 7p13 • LOD score > 2, 9q33.3
Candidate gene study • Case-control • Compare samples • Ethnicity • Associated characteristic or disorder • Family-based • Compare children and their parents or siblings
Dopamine, cognition and behaviour • Neurotoxin reduces DA in rats • hyperlocomotion, learning problems • DA depletion impairs working memory • Impulsiveness associated with low extracellular DA • Blocking DA reuptake makes DA more available and improves executive control
Psychostimulants and ADHD • 54 – 75 % adults and children with ADHD responds to methylphenidate (0.6 mg/kg) • (Spencer et al 2001) • The behavioural modifications induced by stimulants occurs with the reaching of peak plasma level
Dopamine Transporter • Some individuals with ADHD, have higher expression of the dopamine transporter. • Possible mechanism of genetic susceptibility is over expression of the DAT protein • Stimulants blockade dopamine transporter and temporarily correct the levels of dopamine. • DAT Knock Out mouse • difficulty shifting - perseverative errors • novelty-driven hyperactivity • spatial learning deficit
Synaptosomal-Associated Protein of 25 kDa (SNAP-25) Rationale:mouse irradiation mutant strain Coloboma has a single copy of the SNAP-25 gene. The other copy has been deleted. 1) hyperactive 2) responsive to dextroamphetamine 3) not responsive to methylphenidate 4) delayed in some developmental milestones
A number of Genes Identified as linked to ADHD What now? • Confirm linkage in larger samples • Determine how these genes contribute to ADHD • Additional candidates e.g., neurotrophic factors
Neuroimaging • Computed tomography (CT) • Series of x rays from different angles • Positron emission tomography (PET) • Inject radioisotope that emits positrons • Water labelled with oxygen-15 measure changes in blood flow • Deoxyglucose labelled with florine-18 which accumulates in active cells • Magnetic resonance imaging (MRI) • Magnets detect magnetic molecules • fMRI detects changes in magnetic properties of hemoglobin as it carries O2 to active brain cells
Inhibitory control • Withholding and withdrawing of responses if intention or circumstances change or error is made • Failure of inhibition results in errors & impulsiveness
Inhibition and ADHD • Activates orbital, DLPF and basal ganglia • Rich in DA • Disruption of DA by knock out or neurotoxins affects executive control • DA tone associated with executive control • Impulsiveness associated with low extracellular DA • Blocking DA (mostly in basal ganglia) reuptake makes DA more available and improves executive control
Stop Signal Task * fixation point X/O go stimulus: choice reaction time task 500 ms motor response 1000 ms Inter-trial interval = 3000 ms
Stop Signal Task * X/O stop signal delay (variable) 500 ms RED SCREEN or TONE stop signal 1000 ms 500 ms
Latency of inhibition (SSRT) in ADHD and controls SSRT (ms) Schachar et al., 2001
Inhibition & psychopathology • IQ, age, aggression, speed, reading Osterlaans et al., 1999
Inhibition and Methylphenidate Response T-score (Mean = 50, SD = 10) Tannock, Schachar & Logan, 1995
Inhibition in concordant and discordant siblings SSRT ms Concordant Disconcordant Controls
Evidence of performance monitoring • Introspection • Slowing following errors • Slowing following correct responses • Self-detected action slips or errors due to faulty knowledge (external feedback) • Pattern seen in range of tasks • Speeded choice response tasks • Memory tasks • Inhibition tasks
Relevance of performance monitoring to ADHD • Poorly regulated behaviour • “often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities” • Inaccurate and variable task performance
Executive control summary • New breed of measures of specific processes • Cognitively and neurally distinct, multiple deficits characteristic of ADHD • Functional assessment warranted
What do you mean “Cognitive tests are not diagnostic”? • Clinic sample (N = 100) ADHD controls 50/25 50/5 Of 30 cases with “diagnostic marker”, 25/30 =83% will be ADHD • General population (N = 100) ADHD controls 5/2.5 95/19 Therefore, of every 21.5 cases with the “diagnostic marker”, 19/21.5 = 88% will be controls!