Download
1 / 34
340 likes | 2.32k Vues
PELVIC INFECTIONS & URINARY TRACT INFECTION. DR. AKINWUNMI L. AKINWUNTAN MBBS (Ibadan), MHS Pop. & RH (Ibadan), FMCOG (Nig), FWACS OBSTETRICIAN & GYNAECOLOGIST. INTRODUCTION.

E N D
PELVIC INFECTIONS & URINARY TRACT INFECTION DR. AKINWUNMI L. AKINWUNTAN MBBS (Ibadan), MHS Pop. & RH (Ibadan), FMCOG (Nig), FWACS OBSTETRICIAN & GYNAECOLOGIST
INTRODUCTION • Pelvic inflammatory disease (or disorder) (PID) is a term for inflammation of the uterus, fallopian tubes, and/or ovaries • It progresses to scar formation with adhesions to nearby tissues and organs • PID is a vague term and can refer to viral, fungal, parasitic, though most often bacterial infections
STI or STD is often the cause, many other routes are possible, including lymphatic, postpartum (miscarriage or abortion) or intrauterine device (IUD) related, and hematogenous spread
The term "sexually transmitted diseases" is used to denote disorders spread principally by intimate contact • Although this usually means sexual intercourse, it also includes close body contact, kissing, cunnilingus, anilingus, fellatio, mouth–breast contact, and anal intercourse
EPIDEMIOLOGY • In the United States , more than 750,000 women are affected by PID each year, and the rate is highest with teenagers and first time mothers • PID causes over 100,000 women to become infertile in the US each year • About 2% of young women in the UK give a history of PID if asked, and about 1 in 50 consultations with general practitioners made by young women relate to PID
EPIDEMIOLOGY • RISK FACTORS: • Young age • Multiple sex partners • Lack of condom use • Low Socio-economic class • Blacks/Caribbean origin • Genetics- HLA subtype A31 compared with HLA DQA 0501 and DQB 0402 • ??? Bacterial Vaginosis • Indiscriminate/Improper use of antibiotics
Organisms associated with Pelvic inflammatory disease Aerobic • Neisseriagonorrhoeae • Chlamydia trachomatis The big two • Ureaplasmaurealyticum • Mycoplasmagenitalium • Gardnerellavaginalis • Strep. pyogenes • Escherichia coli • Haemophilusinfluenzae • Mycoplasmahominis • Strep. pneumoniae • Mycobacterium tuberculosis
Anaerobic • Bacteroides sp. • Peptostreptococcus sp. • Clostridium bifermentans • Fusobacterium sp. Viruses • Herpes simplex • Echovirus • Coxsackie
NEISSERIA GONORRHOEAE • Neisseriagonorrhoeae is a gram negative diplococcus • Can be seen on microscopy as pairs of red kidney-shaped organisms mostly sitting within polymorphs • Isolated in 40–60% of women with acute salpingitis • It initially infects the cervix but ascends the upper genital tract in 10 -20% of untreated cases
SYMPTOMS & SIGNS • Most women with gonorrhea are asymptomatic • When symptoms occur, they are localized to the lower genitourinary tract and include: • vaginal discharge, urinary frequency or dysuria, and rectal discomfort • Vulva/Vaginal itching • The incubation period is only 3–5 days • Bartholinitis • Acute Pharyngitis/Tosillitis
Purulent vaginal discharge. • Urinary frequency and dysuria • Recovery of organism in selective media • May progress to pelvic infection or disseminated infection • The organism may be recovered from the urethra, cervix, anal canal, or pharynx
Polyathralgia • Tenosynovitis • Dermatitis • Conjunctivitis Opthalmia Neonatorum
Male Urethral Discharge • Discharge coming from the urethral meatus • May be frank pus, mucopurulent, or serous (clear) • Occasionally discharge will be white in colour Gonococcal urethral discharge
DIAGNOSIS • Discharge – Urethral, Cervical, Anal, Pharynx • Thayer-Martins Media • Gram Negative Diplococci in leucocytes • ELISA • Nucleic Acid Amplification Test (NAATs)
CHLAMYDIA TRACHOMATIS • Is estimated to be the cause in about 60% of cases of salpingitis which may lead to PID • Chlamydiae are obligate intracellular microorganisms that have a cell wall similar to that of gram-negative bacteria • They are classified as bacteria and contain both DNA and RNA • Like viruses they grow intracellularly
CLINICAL PRESENTATION • ASYMPTOMATIC • FEVER • ABNORMAL VAGINAL DISCHARGE • LOWER ABDOMINAL PAIN • PAINFUL INTERCOURSE • IRREGULAR MENSTRUAL BLEEDING • PAINFUL MENSTRUATION • CERVICAL MOTION TENDERNESS • COMPLICATION ie Infertility
DIAGNOSIS • Based solely on lab test • Cell Culture isolation: sensitivity= 70-90% • Complement Fixation Methods • Immunofluorescence • DNA Probe
Genital Ulcer Disease Syphilis Chancroid Herpes Simplex
PHYSICIANS’ ROLE • Understand the microbiology of STDs in order to appropriately diagnose and treat patients • To alleviate the symptoms and prevent future sequelae • To prevent the transmission to others including health care professionals • To do all of the above combined with patient education and counseling
Essential Steps In STI Care Management* Syndrome Assessment Contact tracing Compliance Confidentiality Condom use Counseling (diagnostic tools) 5Cs Diagnosis Treatment (screening tests) Risk Assessment
ANTIBIOTIC Rx • CEPHALOSPORINS • Cefuroxime • Ceftriaxone • Cefpodoxime eg Orelox • MACROLIDES • Azithromycin • TETRACYCLINS • Doxycycline • FLUOROQUINOLONES • Ciprofloxacin, Levofloxacin, Ofloxacin
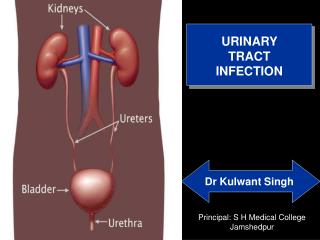
URINARY TRACT INFECTION • A urinary tract infection (UTI) is a bacterial inflammation in the urinary tract • Urethritis - Urethra • Cystitis – Bladder • Pyelonephritis - Kidneys
Risk factors • Women • Anatomy • Sexual intercourse • Pregnancy • Catheterization • Bladder/Kidney stones • Immunosuppression • Stroke/Bedridden • Family history • Diabetes Mellitus
CAUSES • E. Coli - 80 – 85% • Klebsiella • Pseudomonas • Proteus • Enterobacter • Rarely – Viruses and Fungi
SYMPTOMS & SIGNS • Lower Tract • Burning sensation on micturition • Frequency • Urgency • Upper Tract • Flank Pain • Fever • Haematuria/Pyuria • Nausea and Vomiting • Plus symptoms of the lower tract
SYMPTOM & SIGNS….. • In the Elder Post-menopausal • Incontinence • Altered sensorium • Fatigue • Sepsis • Plus earlier symptoms
DIAGNOSIS • HISTORY • LAB: • Urinalysis – Nitrites, Leucocytes, LeucocyteEsteraces • Urine m/c/c – WBCs, RBCs, Bacteria, Colony count ≥ 10,000/colony forming unit Asymptomatic bacteriuria : No symptom plus significant count
TREATMENT • UNCOMPLICATED • Oral Antibiotics • Cephalosporins eg Cefuroxime (Axacef) • Quinolones eg Ciprofloxacin (Cyplox) • Usually a 3-5 day course is sufficient • PYELONEPHRITIS • Requires prolonged medication – Parenteral • Ceftriaxone • Amoxicillin/Clavulanate