Download
1 / 35
370 likes | 466 Vues
Regulation of respiration. Nervous system: Normally adjusts the rate of alv. vent. almost exactly to the demands of the body so that arterial P O2 & P CO2 are hardly altered even during respir. Stress (exercise). Regulation of respiration. Respiratory centre:

E N D
Regulation of respiration Nervous system: • Normally adjusts the rate of alv. vent. almost exactly to the demands of the body so that arterial PO2 & PCO2 are hardly altered even during respir. Stress (exercise)
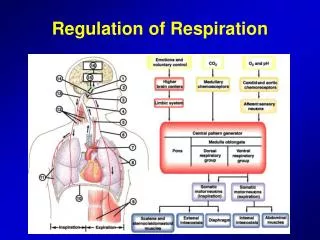
Regulation of respiration • Respiratory centre: neurons in the medulla oblongata and pons of the brain stem divided into: 1- dorsal respiratory group 2- ventral respiratory group 3- pneumotaxic centre 4- apneustic center & pre-Botzinger complex
Regulation of respiration • Dorsal respiratory group: extends through most of the length of the medulla sensory termination of vagal & glossopharyngeal nerves then transmit sensory signals into the respiratory centre signals received from: 1- peripheral chemoreceptors 2- various receptors in the lungs
Regulation of respiration • Rhythmical inspiratory discharge from the dorsal group basic respiratory rhythm is generated in the dorsal group (pre-potzinger complex) this group still emits repetitive bursts of inspiratory neuronal action potentials even if: a- all the peripheral nerves entering the medulla are cut b- the medulla is sectioned from above or below
Regulation of respiration • Inspiratory “ramp” signals : inspiratory signals to the diaphragm are not instantaneous bursts of action potentials normally the signal begins weak and increases steadily in a ramp manner for 2 secs. after that the signal ceases for 3 secs. this causes steady increase in lungs volume and not inspiratory gasps
Regulation of respiration • “Ramp” is controlled by 2 ways: a- control the rate of increment of “ramp” signals. during heavy respiration, “ramp” increases rapidly and fills the lungs b- control the limiting point at which the ramp suddenly ceases. early cease shorter inspiration shorter expiration increased frequency
Regulation of respiration • Pneumotaxic centre: located dorsally in the nucleus parabrachialis of the upper pons transmits signals to the inspiratory center controls the “switch off” point of the inspiratory ramp controlling the duration of the filling phase when weak filling takes 5 secs. when strong filling lasts for 0.5 sec. so the respiratory cycle varies 3-40 breaths/min
Regulation of respiration • Ventral group: located in each side of the medulla 5mm lateral & anterior to the dorsal group functions: 1- inactive during normal quite resp. 2- not involved in the basic rhythmical oscillation 3- provides extra resp. drive when ventilation is more than normal 4- contributes in both inspiration & respiration
Regulation of respiration • The Hering-Breuer inflation reflux: sensory signals from the lungs help in controlling respiration stretch receptors that are found in the muscular portion of the bronchi & bronchioles send their signals with the vagus to the dorsal group these signals are: a- sent when the lungs are overstretched b- have similar effect to that of the pneumotaxic centre c- activated when T.V is larger than 1.5L/breath
Regulation of respiration Chemical control • In order to control [O2], [CO2], [H+] in tissues • Control by CO2 & H+: the chemosensitive respiratory centre is not affected directly by [CO2] . located 0.2mm beneath the surface of the ventral medulla highly sensitive to changes in blood PCO2 or [H+]
Regulation of respiration • Control by CO2 & H+: H+ is likely the primary stimulus for these receptors H+ cannot cross the blood-brain barrier so changes in blood [H+] wont affect these receptors instead an increment in blood PCO2 will indirectly activate these receptors when [CO2] ↑ in blood ↑ in CSF CO2+H2O Carbonic acid bicarbonate + H+
Regulation of respiration • Effect of CO2 on chemosensitive neurons: the excitation effects peaks the 1st hours after the increment in blood [CO2] after 2 days the effect is decreased because of: a- renal adjustment of [H+]. b- increased bicarbonate ions that enter the CSF and bind to H+
Regulation of respiration • O2 effect: virtually no direct effect on respiratory centre because: 1- change of PO2 from 60mmHg to 100mmHg has no effect on the amount of [O2] because of Hb buffering 2- [CO2] in blood & tissue is inversely proportional to the ventilation rate so evolution has made CO2 the major controller instead of O2
Regulation of respiration • Peripheral chemoreceptors: special nervous chemical receptors for detecting changes in O2 in blood & tissues, and to less extent changes in CO2 & H+ carotid bodies (through glossopharyngeal) & aortic bodies (through vagus) to the dorsal group the blood flow supplying these bodies is 20x their weight each minute so the % of removed O2 from the blood flow is virtually zero those bodies are exposed to arterial blood not venous blood
Regulation of respiration • Peripheral chemoreceptors: are stimulated by ↓ [O2], and the range of sensitivity is between 30-60 mmHg (a range in which Hb saturation decreases rapidly)
Regulation of respiration • Effect of CO2 & H+ : ↑ [CO2], [H+] excite receptors ↑respiration both have 7x more effect on the central receptors than on the peripheral receptors but 5x as rapid on the peripheral ones. • Effect of O2: low [O2] excites peripheral receptors “glomus cells” that synapse directly or indirectly with nerve endings. low PO2 and normal [CO2], [H+] will drive the ventilatory process quite strongly
Regulation of respiration • Acclimatization “Chronic breathing of low O2”: Mountain climbers ascend slowly over a period of days causing deep breathing and withstanding low PO2 because after 2 days 4/5th of the sensitivity of receptors to CO2 an H+ is lost so low [O2] ↑ventilation by 400% whereas acute exposure of low [O2] will only ↑ventilation by 70%
Regulation of respiration • Regulation during exercise: In exercise O2 consumption and CO2 formation is increased 20x the ventilation is increased so PO2, PCO2 and pH remain Normal when the brain sends its signals to the muscles it also send collateral signals to the brain stem to increase ventilation even before exercise then chemical factors play a significant role to maintain [O2],[CO2]
Regulation of respiration • Other factors affecting respiration: 1- voluntary control : for short period of times 2- irritant receptors: stimulated by many incidents coughing & sneezing 3- J receptor in alveolar walls lead to edema where the patient has dyspnea 4- brain edema causes res. centre depression 5- anesthesia & narcotic overdose depresses res. centre (halothane, morphine, pentobarbital)
Regulation of respiration • Periodic “Chyne-Stokes” breathing : person over-breathes ↑[O2],↓[CO2] after seconds these [ ] are sensed by the resp. centre inhibition of excess ventilation opposite cycle begins ↓[O2],↑[CO2] after seconds these [ ] are sensed by the resp. centre the person is again over-breathing
Regulation of respiration • Periodic “Chyne-Stokes” breathing : this cycle doesn’t occur normally but can be seen in these conditions: 1- increased neg. feedback gain in resp. control areas change in [CO2], [H+] causes further great change in ventilation “brain-damage” 2- long delay in transporting blood from the lungs to the brain “severe or chronic heart failure,
Regulation of respiration • Sleep apnea: episodes of apnea lasting for 10 secs. Or more, occurring 300-500 times/night Obstructive sleep apnea: during sleep the pharynx is relaxed, in some individuals this may lead to complete closure snoring & labored breathing apnea↓O2,↑CO2 stimulation of resp. center sudden snorts and gasps
1- elderly, obese, nasal ostruction, large tongue, enlarged tonsils 2- Sudden infant death syndrome (SIDS): exaggerated case of sleep apnea, premature baby, smoker pregnant mother
Treatment of obstructive sleep apnea • 1-Surgery uvulopalatopharyngoplasty (remove excess fat at back of throat , tonsils, tracheostomy) • 2-Continous positive airway pressure CPAP