Download
1 / 1
10 likes | 537 Vues
Conditional Job Offer Date: ______________________________________ Start Date: ____________________________________________________ (Start date should be five (5) working days after offer date) Employee’s Anticipated Time of Arrival for Test: ______________ AM PM

E N D
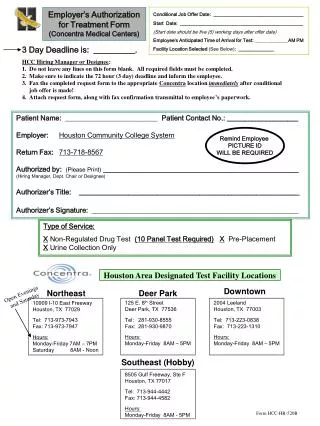
Conditional Job Offer Date: ______________________________________ Start Date: ____________________________________________________ (Start date should be five (5) working days after offer date) Employee’s Anticipated Time of Arrival for Test: ______________AM PM Facility Location Selected (See Below): _______________ Employer’s Authorization for Treatment Form (Concentra Medical Centers) 3 Day Deadline is: __________. HCC Hiring Manager or Designee: 1. Do not leave any lines on this form blank. All required fields must be completed. 2. Make sure to indicate the 72 hour (3 day) deadline and inform the employee. 3. Fax the completed request form to the appropriate Concentra location immediately after conditional job offer is made! 4. Attach request form, along with fax confirmation transmittal to employee’s paperwork. Patient Name: __________________________ PatientContact No.: ____________________ Employer:Houston Community College System Return Fax:713-718-8567 Authorized by:(Please Print) _______________________________________________________(Hiring Manager, Dept. Chair or Designee) Authorizer’s Title: ______________________________________________________________ Authorizer’s Signature: __________________________________________________________ Remind Employee PICTURE ID WILL BE REQUIRED Type of Service: XNon-Regulated Drug Test (10 Panel Test Required)X Pre-Placement X Urine Collection Only Houston Area Designated Test Facility Locations NortheastDeer Park Downtown Open Evenings and Saturday 125 E. 8th Street Deer Park, TX 77536 Tel: 281-930-8555 Fax: 281-930-9870 Hours: Monday-Friday 8AM – 5PM 2004 Leeland Houston, TX 77003 Tel: 713-223-0838 Fax: 713-223-1310 Hours: Monday-Friday 8AM – 5PM 10909 I-10 East Freeway Houston, TX 77029 Tel: 713-973-7943 Fax: 713-973-7947 Hours: Monday-Friday 7AM – 7PM Saturday 8AM - Noon Southeast (Hobby) 8505 Gulf Freeway, Ste F Houston, TX 77017 Tel: 713-944-4442 Fax: 713-944-4582 Hours: Monday-Friday 8AM - 5PM Form HCC-HR-520B